
To evaluate the profile of patients with disc edema/ papilledema and their presenting pattern
Abstract
Background: Raised intracranial pressure (ICP) is a potentially life threatening condition, which can also lead to visual loss and blindness. One of the only objective signs accessible during physical examination to confirm a suspicion of raised ICP is papilledema, or swelling of the optic nerve head (ONH).
Material & Methods: The present study is a non randomized prospective case series being conducted in the 50 patients with disc edema/papilledema attending OPD and referred from other departments to DEPARTMENT OF OPHTHALMOLOGY, Gandhi Medical College and associated Hamidia Hospital, Bhopal from January 2013- December 2014. All patients underwent a complete medical evaluation including careful history taking, ophthalmic examination, complete blood count, blood sugar,urea,creatinine, serum lipid profile, thyroid, chest x-ray in specific cases. and CSF analysis (including opening pressure), follow up examination was compared with fundal photography.
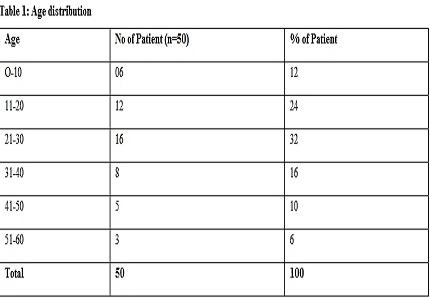
Results: In our study out of 50 patients, Most commonly affected age group was between 21-30 years in which 32% cases were observed, 42% affected were males and 58% females. Papilledema in 30% patient were of local cause in which 22% cases were of optic neuropathy followed by 6% cases of AION in age group of 51-60 year followed by 2% cases of BRAO in age group of 41-40 years. Among systemic causes, 24% cases of ICSOL followed by 12% cases of meningitis, 10% cases of malignant hypertension, 8% cases of drug history, 6% cases of malaria and 2% case each of diabetes, pseudotumorcerebri, anaemia, encephalopathy and head injury.
Conclusion: ophthalmic evaluation and subjective grading of papilledema by FUNDAL examination has the potential of being a low cost objectively and quantitatively, and assess progression and efficacy of treatment directed toward lowering ICP and thus improve clinical decision-making regarding its diagnosis and treatment papilledema.
Downloads
References
2. Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991 Feb;114 ( Pt 1A):155-80. [PubMed]
3. Corbett JJ. The first Jacobson Lecture. Familial idiopathic intracranial hypertension. J Neuroophthalmol. 2008 Dec;28(4):337-47. doi: 10.1097/WNO.0b013e31818f12a2.
4. O'Duffy D, James B, Elston J. Idiopathic intracranial hypertension presenting with gaze-evoked amaurosis. Acta Ophthalmol Scand. 1998 Feb;76(1):119-20.
5. Corbett JJ, Savino PJ, Thompson HS, Kansu T, Schatz NJ, Orr LS, Hopson D. Visual loss in pseudotumorcerebri: follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol. 1982;39:461–474.http://www.ncbi.nlm.nih.gov/pubmed
6. Orcutt JC, Page NG, Sanders MD. Factors affecting visual loss in benign intracranial hypertension. Ophthalmology. 1984 Nov;91(11):1303-12.
7. Radhakrishnan K, Thacker AK, Bohlaga NH, Maloo JC, Gerryo SE. Epidemiology of idiopathic intracranial hypertension: a prospective and case-control study. J Neurol Sci. 1993 May;116(1):18-28. [PubMed]
8. Rowe FJ, Sarkies NJ. Assessment of visual function in idiopathic intracranial hypertension: a prospective study. Eye (Lond). 1998;12 ( Pt 1):111-8. [PubMed]
9. Cameron AJ. Marked papilloedema in pulmonary emphysema. Br J Ophthalmol. 1933 Mar;17(3):167-9. [PubMed]
10. Binder DK, Horton JC, Lawton MT, McDermott MW. Idiopathic intracranial hypertension. Neurosurgery. 2004 Mar;54(3):538-51; discussion 551-2. [PubMed]
11. Menke MN, Feke GT, Trempe CL. OCT measurements in patients with optic disc edema. Invest Ophthalmol Vis Sci. 2005 Oct;46(10):3807-11. [PubMed]
12. Trick GL, Vesti E, Tawansy K, Skarf B, Gartner J. Quantitative evaluation of papilledema in pseudotumor cerebri. Invest Ophthalmol Vis Sci. 1998 Sep;39(10):1964-71. [PubMed]
13. Rebolleda G, Munoz-Negrete FJ. Follow-up of mild papilledema in idiopathic intracranial hypertension with optical coherence tomography. Invest Ophthalmol Vis Sci. 2009;50:5197–5200.
14. Frisén L. Swelling of the optic nerve head: a staging scheme. J Neurol Neurosurg Psychiatry. 1982 Jan;45(1):13-8. [PubMed]
15. Scott CJ, Kardon RH, Lee AG, Frisen L, Wall M. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs clinical expert assessment using a clinical staging scale. Arch Ophthalmol. 2010;128:705–711. [PubMed]
16. Killer HE, Jaggi GP, Miller NR. Papilledema revisited: is its pathophysiology really understood? Clin Experiment Ophthalmol. 2009 Jul;37(5):444-7. doi: 10.1111/j.1442-9071.2009.02059.x.
17. Friedman DI. Papilledema. In: Miller NR, Newman NJ. Walsh and Hoyt’s Clinical Neuro-Ophthalmolgy, 6th Ed.Baltimore: Lippincott Williams and Wilkins, 2005: 237-291.
18. Agarwal, A, Yadav P. Papilledema (choked disc) Journal, Indian Academy of Clinical Medicine _ Vol. 1, No. 3 _ October-December 2000.
19. Julayanont P, Karukote A2, Ruthirago D1, Panikkath D3, Panikkath R3. Idiopathic intracranial hypertension: ongoing clinical challenges and future prospects. J Pain Res. 2016 Feb 19;9:87-99. doi: 10.2147/JPR.S60633. eCollection 2016.
20. Passi N, Degnan AJ, Levy LM. MR imaging of papilledema and visual pathways: effects of increased intracranial pressure and pathophysiologic mechanisms. AJNR Am J Neuroradiol. 2013 May;34(5):919-24. doi: 10.3174/ajnr.A3022. Epub 2012 Mar 15.
21. Bidot S, Bruce BB, Saindane AM, Newman NJ, Biousse V. Asymmetric papilledema in idiopathic intracranial hypertension. J Neuroophthalmol. 2015 Mar;35(1):31-6. doi: 10.1097/WNO.0000000000000205.
22. Maxner CE, Freedman MI, Corbett JJ. Asymmetric papilledema and visual loss in pseudotumour cerebri. Can J Neurol Sci. 1987 Nov;14(4):593-6. [PubMed]
23. Brosh K, Strassman I. Unilateral papilledema in pseudotumor cerebri. Semin Ophthalmol. 2013 Jul;28(4):242-3. doi: 10.3109/08820538.2013.768677. Epub 2013 Apr 29.
24. Wattamwar PR, Baheti NN, Radhakrishnan A. Idiopathic intracranial hypertension presenting as unilateral papilledema. Neurol India. 2010 Sep-Oct;58(5):818-9. doi: 10.4103/0028-3886.72208.
25. Carta A, Favilla S, Prato M, Bianchi-Marzoli S, Sadun AA, Mora P. Accuracy of funduscopy to identify true edema versus pseudoedema of the optic disc. Invest Ophthalmol Vis Sci. 2012 Jan 3;53(1):1-6. doi: 10.1167/iovs.11-8082. [PubMed]
26. Brettschneider J, Hartmann N, Lehmensiek V, Mogel H, Ludolph AC, Tumani H. Cerebrospinal fluid markers of idiopathic intracranial hypertension: is the renin-angiotensinogen system involved? Cephalalgia.2011;31(1):116–121.http://www.ncbi.nlm.nih.gov/pubmed
27. Digre KB, Corbett JJ. Idiopathic intracranial hypertension (pseudotumorcerebri): A reappraisal.Neurologist. 2001;7:2–67. [PubMed]
28. Wang SJ, Silberstein SD, Patterson S, et al. Idiopathic intracranial hypertension without papilledema: A case-control study in a headache center. Neurology. 1998;51:245–249.
29. Vieira DS, Masruha MR, Goncalves AL, et al. Idiopathic intracranial hypertension with and without papilloedema in a consecutive series of patients with chronic migraine. Cephalalgia. 2008;28:609–613.
30. Kleinschmidt JJ, Digre KB, Hanover R. Idiopathic intracranial hypertension: Relationship to depression, anxiety, and quality of life. Neurology. 2000;54:319–324.
31. Friedman DI, Rausch EA. Headache diagnoses in patients with treated idiopathic intracranial hypertension. Neurology. 2002 May 28;58(10):1551-3.
32. Murphy TP. Otologic manifestations of pseudo-tumor cerebri. J Otolaryngol. 1991;20:258–261.http://www.ncbi.nlm.nih.gov/pubmed
33. Rangwala LM, Liu GT. Pediatric idiopathic intracranial hypertension. Surv Ophthalmol. 2007 Nov-Dec;52(6):597-617. [PubMed]
34. Trobe JD. Papilledema: the vexing issues. J Neuroophthalmol. 2011 Jun;31(2):175-86. doi: 10.1097/WNO.0b013e31821a8b0b.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative