
Profile of thyrotoxic patients presenting as pyrexia of unkown origin: An observational case study from a tertiary care hospital
Abstract
Objective: To study the profile of thyrotoxic patients evaluated for pyrexia of unknown origin (PUO).
Methods: 25 patients, who were evaluated for pyrexia of unknown origin and found to have thyrotoxicosis as the cause for fever, were managed as per the recommended protocol and followed for 12 months.
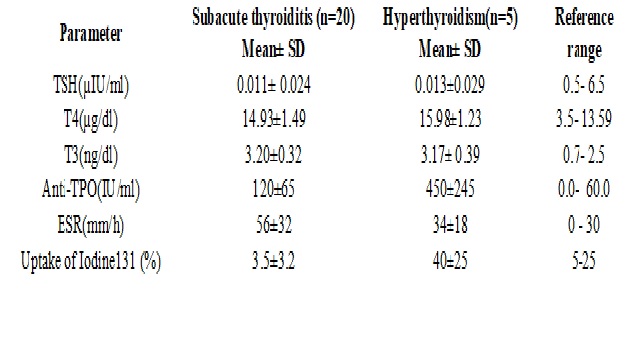
Results: All the patients were presumed to have infectious fever and had received antibiotics prior to diagnosis. Out of 25 patients, 20 (80%) had subacute thyroiditis (SAT) and 5 (20%) had hyperthyroidism (4 had Graves disease and 1 toxic adenoma). Patients with hyperthyroidism received thionamides and β- blockers. 50% patients with subacute thyroiditis received analgesics, 25% received steroids only and 25% received a combination of analgesics and steroids. Early-onset transient hypothyroidism occurred in 40% patients with SAT, permanent hypothyroidism was less common and only 15% of patients were receiving levothyroxine therapy after one year of follow-up.
Conclusion: Thyrotoxicosis should always be included in the differential diagnosis while evaluation of patients with PUO. Most of the patients with thyrotoxicosis are wrongly misinterpreted as infectious PUO and given unnecessary antibiotics. Early-onset transient hypothyroidism is common in SAT compared to permanent hypothyroidism. Although, symptomatic relief is achieved with analgesics and steroids but does not prevent the development of hypothyroidism.
Downloads
References
Phair JP. Fever. Arch Intern Med. 1979 Nov;139(11):1219.
Musher DM, Fainstein V, Young EJ, et al. Fever patterns. Their lack of clinical significance. Arch Intern Med. 1979 Nov;139(11):1225-8.
Aduan RP, Fauci AS, Dale DC, et al. Factitious fever and self-induced infection: a report of 32 cases and review of the literature. Ann Intern Med. 1979 Feb;90(2):230-42.
Buckley RM. Miscellaneous and unusual causes of FUO. In: Murray, H.W. (ed) FUO: Fever of Undetermined Origin. Futura, London. 1983, pp 109-122.
PEO--pyrexia of endocrine origin. Lancet. 1979 Aug 4;2(8136):236-7.
Simon HB, Daniels GH. Hormonal hyperthermia: endocrinologic causes of fever. Am J Med. 1979 Feb;66(2):257-63.
Levine SN. Current concepts of thyroiditis. Arch Intern Med. 1983 Oct;143(10):1952-6.
Dalovisio JR, Blonde L, Cortez LM, Pankey GA. Subacute thyroiditis with increased serum alkaline phosphatase. Ann Intern Med. 1978, 88: 505-507.
Rawson RW. Hyperthyroidism. Disease-a-Month. The Year Book Publishers, Chicago, Apr 1955.
McArthur JW, Rawson RW, Means JH, Cope 0. Thyrotoxic crisis. JAMA.1947, 134: 864-874.
Farwell AP, Braverman LE. Inflammatory thyroid disorders. Otolaryngol Clin North Am. 1996 Aug;29(4):541-56.
Sambit D. Subacute thyroiditis: An uncommon cause of fever of unknown origin. Indian Journal of Endocrinology and Metabolism. 2012;16(8):340-1.
Volpé R, Row VV, Ezrin C. Circulating viral and thyroid antibodies in subacute thyroiditis. J Clin Endocrinol Metab. 1967 Sep;27(9):1275-84.
Kitchener MI, Chapman IM. Subacute thyroiditis: a review of 105 cases. Clin Nucl Med. 1989 Jun;14(6):439-42. Clin Nucl Med. 1989 Jun;14(6):439-42.
Yechiel S, Yecheskel S, Tsila Z. Graves' disease presenting as pyrexia of unknown origin. Postgraduate Medical Journal. 1988(64):209-212.
Raupach T, Karaus M. [Pharyngitis, massive ESR elevation and hyperthyroidism in a 71-year-old female patient]. Internist (Berl). 2004 Oct;45(10):1182-8. DOI: https://doi.org/10.1007/s00108-004-1259-7.
Volpé R. The management of subacute (DeQuervain's) thyroiditis. Thyroid. 1993 Fall;3(3):253-5.
Atkins E, Bodel P. Fever. N Engl J Med. 1972 Jan 6;286(1):27-34. DOI: https://doi.org/10.1056/NEJM197201062860109.
Dinarello CA, Wolff SM. Pathogenesis of fever in man. N Engl J Med. 1978 Mar 16;298(11):607-12.
Simon HB. Extreme pyrexia. JAMA. 1976 Nov 22;236(21):2419-21.
Buckley RM. Miscellaneous and unusual causes of FUO. In: Murray, H.W. (ed) FUO: Fever of Undetermined Origin. Futura, London,.1983, pp 109- 122.
PEO--pyrexia of endocrine origin. Lancet. 1979 Aug 4;2(8136):236-7.
Izmail-Beigi F, Edelman IS. Mechanism of thyroid calorigenesis: role of active sodium transport. Proc Natl Acad Sci U S A. 1970 Oct;67(2):1071-8.
Mcarthur JW, Rawson RW.Thyrotoxic crisis; an analysis of the thirty-six cases at the Massachusetts General Hospital during the past twenty-five years. J Am Med Assoc. 1947 Jul 5;134(10):868-74.
Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003 Jun 26;348(26):2646-55. DOI: https://doi.org/10.1056/NEJMra021194.
Singer PA. Thyroiditis. Acute, subacute, and chronic. Med Clin North Am. 1991 Jan;75(1):61-77.
Chiovato L, Martino E Thyroiditis. In: Pinchera A, ed. Endocrinology and Metabolism. London: Mc Graw-Hill International (UK) Ltd.. 2001: 189–9.
Gozariu L, Stroe M, Vladutiu T, et al. Late hypothyroidism following subacute thyroiditis. Exp Clin Endocrinol. 1986 Jun;87(1):48-52.
Iitaka M, Momotani N, Hisaoka T, et al. TSH receptor antibody-associated thyroid dysfunction following subacute thyroiditis. Clin Endocrinol (Oxf). 1998 Apr;48(4):445-53.
Lio S, Pontecorvi A, Caruso M, et al. Transitory subclinical and permanent hypothyroidism in the course of subacute thyroiditis (de Quervain). Acta Endocrinol (Copenh). 1984 May;106(1):67-70.
Tikkanen MJ, Lamberg BA. Hypothyroidism following subacute thyroiditis. Acta Endocrinol (Copenh). 1982 Nov;101(3):348-53.
Brouqui P, Raoult D, Conte-Devolx B. Coxsackie thyroiditis. Ann Intern Med. 1991 Jun 15;114(12):1063-4.
Volpé R, Row VV, Ezrin C. Circulating viral and thyroid antibodies in subacute thyroiditis. J Clin Endocrinol Metab. 1967 Sep;27(9):1275-84.
Sato M. Virus-like particles in the follicular epithelium of the thyroid from a patient with subacute thyroiditis (De Quervain). Acta Pathol Jpn. 1975 Jul;25(4):499-501.
Tauveron I, Thieblot P, Marcheix JC. Recurrence after 12 years of de Quervain-Crile subacute thyroiditis [French]. Rev Med Interne. 1991;12:396.
Bauman A, Friedman A. Recurrent subacute thyroiditis: a report of three cases. N Y State J Med. 1983 Jun;83(7):987-8.
Iitaka M, Momotani N, Ishii J, et al. Incidence of subacute thyroiditis recurrences after a prolonged latency: 24-year survey. J Clin Endocrinol Metab. 1996 Feb;81(2):466-9.
Yamamoto M, Saito S, Sakurada T, Tamura M, Kudo Y, Yoshida K, Kaise K, Kaise N, Fukazawa H, Itagaki Y, Yoshinaga K. Recurrence of subacute thyroiditis over 10 years after the first attack in three cases. Endocrinol Jpn. 1988;35:833–839.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative