
Clinicopathological profile of mediastinal masses in a tertiary care hospital of Eastern India
Abstract
Introduction:The Mediastinum is the central part of thorax where various organs are located which gives rise to various neoplastic and non- neoplastic lesions.Accurate diagnosis is important to formulate proper therapeutic strategy and predict prognosis. Studies are very few in this part of the country.
Objective: To analyse presentation of patients with Meditastinal Mass and to classify according to the location of mass. Also, to document Malignant versus Non-malignant nature oflesions.
Methods: Total 33 patients with mediastinal masses diagnosed by Imagingand Histopathological study were taken up consecutively in the study during one year of study.
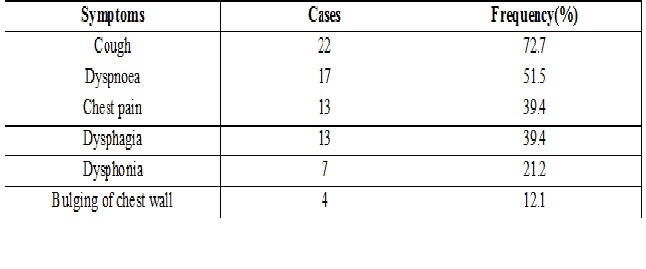
Results: of the 33 cases, 21 were male (63.6%) and 12 were female (36.4%), Male; female ratio being 1.8: 1. Age ranged from 14 years to 72 years maximum of 8 Patients (24.2%) in the 12-20 years of age group. 57% of the masses were malignant and 43% were benign. Most common lesion was Lymphoma in 10 cases (30.3%) followed by8 cases of Thymic tumours (24.2%). Metastatic Carcinoma was found in 6 patients (18.2%) followed by 3 patients of Germ cell tumours.One case each of Neurofibroma, Neurolipoma and 6 are of different less common category. Compartment wise, 9 cases (27.3%) were in Anterior Compartment, 1 (3%) case in Post Compartment, 3 case in superior mediastinum, 6 case in Middle mediastinum. Maximum cases, 14(42.5%) were occupying Multiple Compartments. Most common symptom was cough (72%). Pleural and Pericardial effusions were common complication of malignant lesions contributing 7 out of 19(36%) and 3 out of 19(17%) respectively.
Conclusion: Mediastinal masses creates a diagnostic dilemma to the clinician. Uncommon cause of common symptoms like cough and common presentation of pleural or pericardial effusion may have Mediastinal mass behind the screen.
Downloads
References
Aroor AR, Prakasha S R, Seshadri S, et al. A study of clinical characteristics of mediastinal mass. J Clin Diagn Res. 2014 Feb;8(2):77-80. doi: https://dx.doi.org/10.7860%2FJCDR%2F2014%2F7622.4013. Epub 2014 Feb 3.
Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest. 2005 Oct;128(4):2893-909. DOI: https://doi.org/10.1378/chest.128.4.2893.
Vaziri M, Pazooki A, Zahedi-Shoolami L. Mediastinal masses: Review of 105 cases. Acta Med Iranica 2009; 47(4):297-300.
Adegboye VO, Ogunseyinde AO, Obajimi MO, et al. Presentation of primary mediastinal masses in Ibadan. East Afr Med J. 2003 Sep;80(9):484-7.
Davis RD Jr, Oldham HN Jr, Sabiston DC Jr. Primary cysts and neoplasms of the mediastinum: recent changes in clinical presentation, methods of diagnosis, management, and results. Ann Thorac Surg. 1987 Sep;44(3):229-37.
Dubashi B, Cyriac S, Tenali SG. Clinicopathological analysis and outcome of primary mediastinal malignancies - A report of 91 cases from a single institute. Ann Thorac Med. 2009 Jul;4(3):140-2. doi: https://dx.doi.org/10.4103%2F1817-1737.53354.
Singh G, Amin Z, Wuryantoro, Wulani V, Shatri H. Profile and factors associated with mortality in mediastinal mass during hospitalization at CiptoMangunkusumo Hospital, Jakarta. Indonesian Journal of Internal Medicine.2013; 45:3-10.
Jitendr G Nasit, Maulin Patel, Biren Parikh, Manoj Shah, KajalDavara. Anterior mediastinal masses: A study of 50 Cases by fine needle aspiration cytology and core needle biopsy as a diagnostic procedure. South Asian Journal of Cancer.2013 Jan-March; 2(1):7-13.
Shrivastava CP, Devgarha S, Ahlawat V. Mediastinal tumors: a clinicopathological analysis. Asian CardiovascThorac Ann. 2006 Apr;14(2):102-4. DOI: https://doi.org/10.1177%2F021849230601400204.
Blegvad S, Lippert H, Simper LB, et al. Mediastinal tumours. A report of 129 cases. Scand J ThoracCardiovasc Surg. 1990;24(1):39-42.
Ramakant Dixit, Narender Singh Shah, Mukesh Goyal, Chetan B Patil, Mukesh Panjabi, Rakesh C Gupta, Neeraj Gupta, SabarigiriVasan Harish. Diagnostic evaluation of mediastinal lesions: Analysis of 144 cases. Lung India 2017;34(4) :341-348. DOI: https://dx.doi.org/10.4103%2Flungindia.lungindia_311_16.
Malatani TS. Primary mediastinal tumours in the southern region of Saudi Arabia. Indian J Chest Dis Allied Sci. 1996 Oct-Dec;38(4):235-9.
Bekele A , Ali A ,Gulilat D , Kassa S , Nega B . Patterns of mediastinal tumors operated at the TikurAnbessa Hospital, Addis Ababa, Ethiopia over a six years period. Ethiopian Medical Journal 01 Apr 2013; 51(2):143-152.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative