
A Study of clinical profile, disease severity and treatment response of Movement disorders at a tertiary care teaching hospital
Abstract
Background: Movement disorders are one of the common neurological problems seen by General physicians and neurophysicians. The clinical phenotype of Movement disorders is variable.
Aim of the study: The objective of the study was to study the clinical profile, disease severity and treatment response of Movement disorders at a tertiary care teaching hospital.
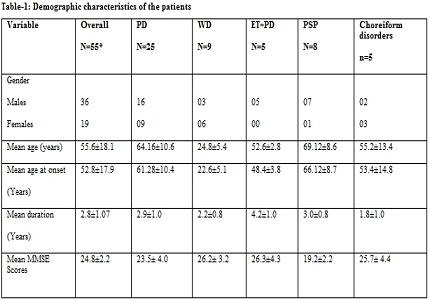
Results: The present study was a prospective observational study comprising 55 clinically detectable patients of movement disorders. Out of fifty-five, the frequency of various Movement disorders were as follows: Parkinson’s disease- 25 (45.5%), Wilson`s disease (WD)-9 (16.36%), Progressivesupranuclear palsy- 8(14.54%), Essential Tremor with Parkinson disease 5 (9.0%), Choreiform disorders- 5(9.0%). Mean MDS-UPDRS Part III score in OFF stage of PD was 57.7±13.2 and in ON stage was 28.2±10.2 suggesting significant improvement. Seventy-six percentages of PD patients had Good response to Dopaminergic agonists and Levodopa administration, while better response was seen in WD, ET+PD and the poor response in PSP patients respectively.
Conclusion: Identifying and describing the clinical phenomenology of Movement disorders is the first step in the diagnostic evaluation of the patients as against to the localization in General Neurological disorders. Disease severity scales do assess the progression of the disease at the earliest and there are affordable regimes of various medications are available to treat them at the earliest, so as to reduce the morbidity and to increase health related quality of life.
Downloads
References
Abdo WF, van de Warrenburg BP, Burn DJ, Quinn NP, Bloem BR. The clinicalapproach to movement disorders. Nat Rev Neurol.2010Jan;6(1):29-37. doi: https://doi.org/10.1038/nrneurol.2009.196.
Goetz CG, Tilley BC, Shaftman SR et al. Movement Disorder Society UPDRS Revision Task Force. Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008 Nov 15;23(15):2129-70. doi: https://doi.org/10.1002/mds.22340.
Aggarwal A, Aggarwal N, Nagral A, Jankharia G, Bhatt M. A novel Global Assessment Scale for Wilson's Disease (GAS for WD). Mov Disord. 2009 Mar 15;24(4):509-18. doi: https://doi.org/10.1002/mds.22231.
Spss I. IBM SPSS statistics version 21. Boston, Mass: International Business Machines Corp. 2012:126.
Golbe LI, Ohman-Strickland PA. A clinical rating scale for progressive supranuclear palsy. Brain. 2007 Jun;130(Pt 6):1552-65. Epub 2007 Apr 2.
Dubois B, Slachevsky A, Litvan I, Pillon B.The FAB: a Frontal Assessment Battery at bedside.Neurology. 2000 Dec 12;55(11):1621-6.DOI: https://doi.org/10.1212/WNL.55.11.1621
Elble RJ. The Essential Tremor Rating Assessment Scale.J Neurol Neuromed (2016) 1(4): 34-38.DOI: https://doi.org/10.1002/mds.25162
Antoˆnio Lu ́cio Teixeira, Jr., De ́bora P. Maia, Francisco Cardoso.UFMG Sydenham’s Chorea Rating Scale (USCRS): Reliability and Consistency Movement Disorders Vol. 20, No. 5, 2005, pp. 585–91.DOI: https://doi.org/10.1002/mds.20377.
Toth C, Rajput M, Rajput AH. Anomalies of asymmetry of clinical signs in parkinsonism. Mov Disord. 2004 Feb;19(2):151-7.
Bhidayasiri R. Differential diagnosis of common tremor syndromes. Postgrad Med J. 2005 Dec;81(962):756-62.
Jankovic J, Schwartz KS, Ondo W. Re-emergent tremor of Parkinson's disease. J Neurol Neurosurg Psychiatry. 1999 Nov;67(5):646-50.
Jankovic J:Pathophysiology and clinical assessment of Parkinsonian symptoms and signs. In Pahwa R,Lyons K, Koller WC (ed):Handbook of Parkinsons disease.New York,Marcel Dekker,2003,pp71-107.
Winkler AS, Reuter I,Harwood G,Chaudhuri KR: The frequency and significance of striatal toe in Parkinsonism.Parkinsonism Relat Disord 2002;9:97-101.PMID:12473399
Brooks DJ, Pavese N. Imaging non-motor aspects of Parkinson's disease. Prog Brain Res. 2010;184:205-18. doi: https://doi.org/10.1016/S0079-6123(10)84011-7.
Ibarretxe-Bilbao, N., Junque, C., Marti, M. And Tolosa, E. Brain structural MRI correlates of cognitive dysfunctions in Parkinson’s disease. J NeurolSci 2011a 310: 70–74.DOI: https://doi.org/10.1016/j.jns.2011.07.054. Epub 2011 Aug 23.
Svenningsson P, Westman E, Ballard C, Aarsland D. Cognitive impairment in patients with Parkinson's disease: diagnosis, biomarkers, and treatment. Lancet Neurol. 2012 Aug;11(8):697-707. doi: https://doi.org/10.1016/S1474-4422(12)70152-7.
Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson's disease. N Engl J Med. 2005 Sep 8;353(10):1021-7.
Ferreira JJ, Katzenschlager R, Bloem BR et al. Summary of the recommendations of the EFNS/MDS-ES review on therapeutic management of Parkinson's disease. Eur J Neurol. 2013 Jan;20(1):5-15. doi: https://doi.org/10.1111/j.1468-1331.2012.03866.x.
Grimes D, Gordon J, Snelgrove Bet al. Canadian Nourological Sciences Federation. Canadian Guidelines on Parkinson's Disease. Can J Neurol Sci. 2012 Jul;39(4 Suppl 4):S1-30.
Miyasaki JM, Martin W, Suchowersky O, Weiner WJ, Lang AE. Practice parameter: initiation of treatment for Parkinson's disease: an evidence-based review: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2002 Jan 8;58(1):11-7.
Fahn S. Levodopa in the treatment of Parkinson's disease. J Neural Transm Suppl. 2006;(71):1-15.
Chaudhuri KR, Rizos A, Sethi KD. Motor and nonmotor complications in Parkinson's disease: an argument for continuous drug delivery? J Neural Transm (Vienna). 2013 Sep;120(9):1305-20. doi: https://doi.org/10.1007/s00702-013-0981-5. Epub 2013 Mar 2.
Sawada H, Oeda T, Kuno S, et al. Amantadine for dyskinesias in Parkinson’s disease: a randomized controlled trial. PLoS One. 2010;5(12):e15298.DOI: https://doi.org/10.1371/journal.pone.0015298.
Ory-Magne F, Corvol JC, Azulay JPet al. NS-Park CIC Network. Withdrawing Amantadine in dyskinetic patients with Parkinson disease: the AMANDYSK trial. Neurology. 2014 Jan 28;82(4):300-7. doi: https://doi.org/10.1212/WNL.0000000000000050. Epub 2013 Dec 26.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative