
Unusual presentation of interrupted aortic arch: a case report and radiological review
Abstract
Interrupted aortic arch, arare congenital malformation and there is a loss of luminal continuity between the ascending and descending portions of the aortic arch. Their incidences are of 3 per million live births and manage by surgical treatment. Till now only 12 cases of isolated interrupted aortic arch reported in adults. We notify the computed tomography imaging findings of a 29-year-old femalepatients presented to our hospital. MDCT has advantages of a less scanning time with more spatial resolution and high temporal resolution. Fine anatomic structures can be evaluated by retrospective reconstruction. Within few years MDCT has become a primary diagnostic tool for evaluation of aortic abnormality. Volumetric scanning of chest done in 64 slices MDCT with plain and contrast enhanced (I.Vnon-ionic) contiguous axial images taken from chest and evaluated in appropriate window settings.
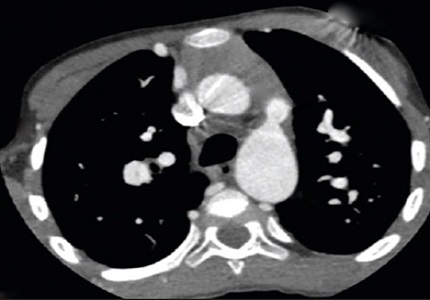
Result: Multi-detector computed tomography (MDCT) angiography with a 64 slice MDCT were performed. The aortic arch is seen interrupted, approx. 1.8cm long segment of aortic arch just after the origin of subclavian artery is not seen (absent), thick chunk of irregular calcification is seen in the region of termination of aortic arch. Descending thoracic aorta is smaller in caliber measure approx. 1.1 x 1.2 cm in diameter & shows well luminal contrast opacification. Prominent Para vertebral collaterals seen suggesting collateral filling of descending thoracic aorta. No evident contrast filled patent ductus arteriosus seen, a tubular slightly enhancing structure seen in this region.
Downloads
References
Steidele RJ. Sammlung verchiedener in der chirurg. Prakt Lehschule Gemachten Beobb (Viena) 1778;2:114.
Goo HW, Park IS, Ko JK, Kim YH, Seo DM, Yun TJ, Park JJ, Yoon CH. CT of congenital heart disease: normal anatomy and typical pathologic conditions. Radiographics. 2003 Oct;23 Spec No:S147-65.
Pannu HK, Flohr TG, Corl FM, Fishman EK.Current concepts in multi-detector row CT evaluation of the coronary arteries: principles, techniques, and anatomy. Radiographics. 2003 Oct;23 Spec No:S111-25.
CELORIA GC, PATTON RB. Congenital absence of the aortic arch. Am Heart J. 1959 Sep;58:407-13.
Collins-Nakai RL, Dick M, Parisi-Buckley L, Fyler DC, Castaneda AR. Interrupted aortic arch in infancy. J Pediatr. 1976 Jun;88(6):959-62.
Krieger KH, Spencer FC. Is paraplegiaafterrepair of coarctation of the aorta due principally to distalhypotension during aorticcross-clamping?Surgery. 1985 Jan;97(1):2-7.
Yang DH, Goo HW, Seo DM, Yun TJ, Park JJ, Park IS, Ko JK, Kim YH. Multislice CT angiography of interrupted aortic arch. Pediatr Radiol. 2008 Jan;38(1):89-100. Epub 2007 Oct 27.
Dillman JR, Yarram SG, D'Amico AR, Hernandez RJ. Interrupted aortic arch: spectrum of MRI findings. AJR Am J Roentgenol. 2008 Jun;190(6):1467-74. doi: https://doi.org/10.2214/AJR.07.3408.
Reardon MJ, Hallman GL, Cooley DA. Interrupted aortic arch: Brief review and summary of an eighteen-year experience. Tex Heart Inst J 1984;11:250-9.
Ho SY, Wilcox BR, Anderson RH, Lincoln JC. Interrupted aortic arch--anatomical features of surgical significance. Thorac Cardiovasc Surg. 1983 Aug;31(4):199-205.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative