
Double Trouble: an observational study of thyroid dysfunction in South Indian subjects with type 2 diabetes
Abstract
Objective: Studies conducted in subjects with type 2 diabetes have shown increased prevalence of overt hypothyroidism and subclinical hypothyroidism. Hence, we designed a study to find out the prevalence of thyroid dysfunction in south Indian subjects with type 2 diabetes.
Research Design and Methods: 400 subjects with type 2 diabetes attending the out-patient department of Karnataka Institute of Endocrinology and Research, Bangalore were randomly selected. 200 relatives who accompanied the subjects without diabetes were recruited as controls. BMI, waist circumference, blood pressure, fasting plasma glucose, post prandial plasma glucose, HbA1c, lipid profile, and thyroid profile of these subjects were determined.
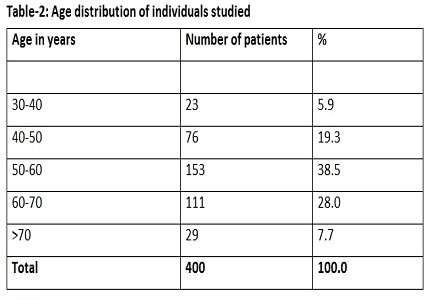
Results: 400 subjects with type 2 diabetes and 200 subjects without diabetes were included in the study. They were in the age group of 25 to 75 years. Thyroid dysfunction was present in 13% of non diabetic controls. Subclinical hypothyroidism was present in 7%, overt hypothyroidism in 5% and hyperthyroidism in 1% of the controls. Thyroid dysfunction was present in 24% of subjects with type 2 diabetes. Subclinical hypothyroidism was present in 11.25%, overt hypothyroidism in 12% and hyperthyroidism in 0.75% of the 400 subjects with type 2 diabetes.
Conclusions: Hypothyroidism especially subclinical hypothyroidism is more common in south Indian subjects with type 2 diabetes. Hence, it is indispensable to investigate for thyroid dysfunction in subjects with type 2 diabetes. Failure to recognize the presence of thyroid dysfunction may be a primary cause of poor glycemic control often encountered in some subjects with type 2 diabetes, despite appropriate anti diabetic therapy. This highlights the need for the routine evaluation of thyroid function in subjects with type 2 diabetes.
Downloads
References
Imani SF, Hashemipour M, Kelishadi R. Lipid profile of children with type in diabetes compared to controls. ARYA Journal. 2006; 2(1):36-8.
World Health Organization (1985). Diabetes mellitus: Report of a WHO study group Technical Report Series 727.
Nam Han Cho et al (2015). IDF Diabetes Atlas Seventh Edition.
Feely J, Isles TE. Screening for thyroid dysfunction in diabetics. British Medical Journal. 1979; 1(6179):1678.
Gray, R.S., Irvine, W.J. and Clarke, B.F. Screening for thyroid dysfunction in diabetics. Br Med J. 1979; 2 (6 202): 1439.
Perros P, McCrimmon RJ, Shaw G, Frier BM. Frequency of Thyroid Dysfunction in Diabetic Patients: Value of Annual Screening. Diabet Med, 1995; 12: 622–627. doi: https://doi.org/10.1111/j.1464-5491.1995.tb00553.x.
Smithson MJ. Screening for thyroid dysfunction in a community population of diabetic patients. Diabet Med, 1998; 15: 148–150. doi: https://doi.org/10.1002/(SICI)1096-9136(199802)15:2%3C148::AID-DIA540%3E3.0.CO;2-H.
Sugrue DD, McEvoy M, Drury MI. Thyroid disease in diabetics. Postgraduate Medical Journal. 1982; 58(685):680-684.
Shah SN. Thyroid disease in diabetes mellitus. J Assoc Physicians India, 2007; 32(12):1057- 1059.
Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, Pessah-Pollack R, Singer PA, Woeber for the American Association of Clinical Endocrinologists and American Thyroid Association Taskforce on Hypothyroidism in Adults KA. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid. 2012; 22(12):1200-35.
DeFronzo RA. Lilly lecture 1987. The triumvirate: beta-cell, muscle, liver. A Collusion responsible for NIDDM. Diabetes 1988; 37:667–687.
DeFronzo RA. Pathogenesis of type 2 diabetes: metabolic and molecular implications for identifying diabetes genes. Diabetes Res 1997; 5:177–269.
Gastaldelli A, Ferrannini E, Miyazaki Y, Matsuda M, DeFronzo RA, San Antonio metabolism study Beta-cell dysfunction and glucose intolerance: results from the San Antonio metabolism (SAM) study. Diabetologia2004;47:3139.
Abdul Ghani MA, Jenkinson CP, Richardson DK, Tripathy D, DeFronzo RA .Insulin secretion and action in subjects with impaired fasting glucose and impaired glucose tolerance: results from the Veterans Administration Genetic Epidemiology Study. Diabetes 2006;55:1430–1435pmid:16644701.
DeFronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes2009;58:773–795pmid:19336687.
Sanjeet Bagcchi Lancet diabetes and endocrinology volume 2 October 2014.
Wang C. The Relationship between Type 2 Diabetes Mellitus and Related Thyroid Diseases. Journal of Diabetes Research. 2013; 2013:390534. doi: https://doi.org/10.1155/2013/390534.
Huber A, Menconi F, Corathers S, Jacobson EM, Tomer Y. Joint genetic susceptibility to type 1 diabetes and autoimmune thyroiditis: from epidemiology to mechanisms. Endocrine Reviews. 2008 Oct; 29(6):697-725.
Ashok Khurana, Preeti Dhoat, Gourav Jain. Prevalence of thyroid disorders in patients of type 2 diabetes mellitus JIACM 2016; 17(1): 12-15.
Navneet Agrawal, Manoj Gulati. Study of prevalence of thyroid dysfunction in patients with type 2 diabetes mellitus. International Journal of Contemporary Medical Research 2016; 3(8):2212-2214.
Demitrost L, Ranabir S. Thyroid dysfunction in type 2 diabetes mellitus: A retrospective study. Indian Journal of Endocrinology and Metabolism. 2012; 16(Suppl 2):S334-S335. doi: https://dx.doi.org/10.4103%2F2230-8210.104080.
Singh G, Gupta V, Sharma AK, Gupta N. Evaluation of thyroid dysfunction among type 2 diabetic Punjabi population. Advances in bioresearch. 2011 Dec 2; 2(2):3-9.
Papazafiropoulou A, Sotiropoulos A, Kokolaki A, Kardara M, Stamataki P, Pappas S. Prevalence of thyroid dysfunction among Greek type 2 diabetic patients attending an outpatient clinic. Journal of clinical medicine research. 2010 Mar 25; 2(2):75-8.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative