
Adrenal histoplasmosis in an immunocompetant Individual– a rare case report
Abstract
Introduction: Disseminated histoplasmosis is common particularly among immunocompromised individuals, alcoholics and extremes of age. It is of concern because of the associated high morbidity and mortality. Asymptomatic adrenal involvement has also been described in 30 to 50 % of patients with disseminated histoplasmosis. We report a case of adrenal histoplasmosis in an immune-competent subject presenting with adrenal insufficiency.
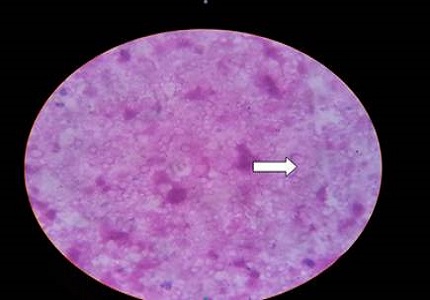
Case Report: A 49 years old Indian male presented with three months history of weakness, nausea and vomiting, mucocutaneous pigmentation and weight loss. Past medical history was significant for tuberculosis, for which he was incompletely treated. He was non-smoker, non-alcoholic and non-diabetic, with no history of sexual promiscuity. USG of abdomen revealed bilateral suprarenal mass, with right adrenal (48.3x 39.3mm) and left adrenal measuring (42.4 x 38mm). CECT scan of upper abdomen showed enlargement of both adrenal glands with right adrenal 44x25x43mm, left adrenal measuring 53x37x46 mm suggestive of adrenal adenoma. CT guided FNAC of right adrenal mass showed necrosis, many budding yeast cells having the morphology of Histoplasma capsulatum. The patient was treated with liposomal form of amphotericin –B 150 mg / day for two weeks followed by oral itraconazole 200mg BD for one year and hydrocortisone 25 mg/day in divided doses. After one month, there was gain in weight, pigmentation faded and nausea & vomiting disappeared.
Conclusion: Adrenal histoplasmosis usually occurs in a setting of immunocompromised condition and in endemic area, but it does occur in immunocompetant hosts from non-endemic area, as in our case. It is prudent to obtain a cytological or histopathological examination to confirm the diagnosis so that appropriate treatment can be instituted to avoid fatal complications.
Downloads
References
Anderson E. Histoplasmosis.. Pediatr Infect Dis J. 2006 Jan; 25(1):73-4.
Panja G and Sen S. A unique case of histoplasmosis. Journal of Indian Medical Association 1954; 23: 257-258. J Indian Med Assoc. 1954 Mar;23(6):257-8.
Goswami RP, Pramanik N, Banerjee D, Raza MM, Guha SK, Maiti PK. Histoplasmosis in eastern India: the tip of the iceberg? Trans R Soc Trop Med Hyg. 1999 Sep-Oct;93(5):540-2.doi: https://doi.org/10.1016/s0035-9203(99)90374-7.
Kumar N, Singh S, Govil S. Adrenal Histoplasmosis: Clinical Presentation and Imaging Features in 9 Cases. Abdominal Imaging, 2003;28:703-8 Kumar N, Singh S, Govil S. Adrenal histoplasmosis: clinical presentation and imaging features in nine cases. Abdom Imaging 2003;28:703-8.doi: https://doi.org/10.1007/s00261-003-0010-5.
Lam KY, Lo CY. Metastatic Tumors of Adrenal Glands: A 30 years Experience in Teaching Hospital. Clinical Endocrinology 56:96-101, 2002. Clin Endocrinol (Oxf). 2002 Jan;56(1):95-101.doi: https://doi.org/10.1046/j.0300-0664.2001.01435.x.
Leal AM, Bellucci AD, Muglia VF, Lucchesi FR. Unique adrenal gland imaging features in Addison's disease caused by paracoccidioidomycosis. AJR Am J Roentgenol. 2003 Nov;181(5):1433-4.doi: https://doi.org/10.2214/ajr.181.5.1811433.
Moreira SG Jr, Pow-Sang JM. Evaluation and management of adrenal masses. Cancer Control. 2002 Jul-Aug;9(4):326-34.doi: https://doi.org/10.1177/107327480200900407.
Fernandes VS, Bisi H, Longatto Filho A, de Camargo RY. [Incidence of adrenalitis in necropsy material]. Rev Hosp Clin Fac Med Sao Paulo. 1991 Sep-Oct;46(5):219-22. https://www.ncbi.nlm.nih.gov/pubmed/1843724.
Rosen bit AM, Kin A, et al, adrenal histoplasmosis manifested as Addison disease. Unusual CT feasures with magnetic resonance imaging correlation. Clinical Radiology 2001; 56:682-4.
Gohar S, Sule A, Gaitonde S, Mittal G, Ejaz P, Mangat G, Bhaduri A, Joshi VR. Adrenal histoplasmosis. J Assoc Physicians India. 2001 Sep;49:916-7. https://www.ncbi.nlm.nih.gov/pubmed/11837763.
Grover SB, Midha N, Gupta M, Sharma U, Talib VH. Imaging spectrum in disseminated histoplasmosis: case report and brief review. Australas Radiol. 2005 Apr;49(2):175-8. doi: https://doi.org/10.1111/j.1440-1673.2005.01369.x.
Fitzhugh VA, Maniar KP, Kim MK, Chen H, Schainker BA. Adrenal histoplasmosis. Diagn Cytopathol. 2010 Mar;38(3):188-9. doi: https://doi.org/10.1002/dc.21080.
Gopal K, Singh S, Gupta R. Fine needle aspiration cytology in bilateral adrenal mass in a 58 years old man. Actacytol 2010;54: 234-6.doi: https://doi.org/10.1159/000325018.
Subramanian S, Abraham OC, Rupali P, Zachariah A, Mathews MS, Mathai D. Dissiminated histoplasmosis. Journal of association physician of India, 2005; 53:185-9. J Assoc Physicians India. 2005 Mar;53:185-9. https://www.ncbi.nlm.nih.gov/pubmed/15926599.
Rana C1, Kumari N, Krishnani N. Adrenal histoplasmosis: a diagnosis on fine needle aspiration cytology. Diagn Cytopathol. 2011 Jun;39(6):438-42. doi: https://doi.org/10.1002/dc.21453. Epub 2010 Oct 14.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative