
Comparison of daily and intermittent anti tubercular treatment in achieving sputum negativity in newly diagnosed sputum positive Pulmonary tuberculosis patients
Abstract
Introduction: Tuberculosis is a major health problem in India. Sputum positive pulmonary tuberculosis patients expel bacilli for a variable period after the start of treatment. The period of infectivity depends on the drugs, dosage and interval period. Achieving sputum negativity helps in reducing secondary cases.
Aim: Comparison of the effectiveness of daily and intermittent anti tubercular treatment in achieving sputum negativity in newly diagnosed sputum positive pulmonary tuberculosis patients without comorbidities.
Methods: A prospective study was carried out in BJMC and SGH, Pune. 71 sputum positive pulmonary tuberculosis patients were included in the study. 35 patients received daily treatment and 36 patients received intermittent treatment. Patients were followed up on 15th, 30th, 45th and 60th day of treatment.
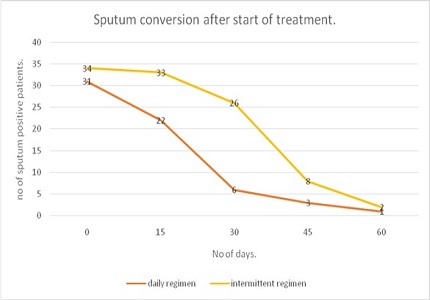
Results: Mean duration of sputum conversion was 29 days in daily treatment and 44 days in intermittent treatment. Patients on daily regimen have sputum conversion about 15 days earlier as compared to intermittent regimen. (p<0.05).
Conclusion: Patients on daily treatment are sputum negative 15 days prior to patients on intermittent treatment. Using daily treatment will decrease the period of communicability. Thus daily treatment will decrease the incidence and prevalence of the disease in a country with heavy burden of tuberculosis. A cost effective approach will be daily treatment during intensive phase and intermittent treatment during continuation phase.
Downloads
References
"Global TB Report". http://www.who.int/tb/publications/global_report, 2015.
"RNTCP India Training Module 1-4". http://www.tbcindia.nic.in, 2010.
Global tuberculosis control surveillance planning financing report, http://www.who.int/tb, 2012.
Srinath S, Sharath B, Santosha K, Chadha SS, Roopa S, Chander K, Wares F, Chauhan LS, Wilson NC, Harries AD. Tuberculosis 'retreatment others': profile and treatment outcomes in the state of Andhra Pradesh, India. Int J Tuberc Lung Dis. 2011 Jan;15(1):105-9.
Tuberculosis Chemotherapy Centre (Indian Council of Medical Research),Chennai. Low rate of emergence of drug resistance in sputum positive patients treated with short-course chemotherapy. Int J Tubercle Lung Dis 2001;5(1):40-45.
Naude TM, Jim M. Twice weekly vs. daily chemotherapy for childhood tuberculosis. Pediatric Infectious Disease Journal:2000;19:405-410.
Parikh R, Nataraj G, Kanade S, Khatri V, Mehta P. Time to sputum conversion in smear positive pulmonary TB patients on category I DOTS and factors delaying it. J Assoc Physicians India. 2012 Aug;60:22-6.
Treatment of tuberculosis guidelines. Technical paper, 5th pacific, Stop TB meeting, Nadi, Fiji, May 2010.
Banu Rekha VV, Balsubramanian R, Swaminathan S. Sputum conversion at the end of intensive phase treatment of pulmonary tuberculosis patients with diabetes mellitus or HIV infection. Indian J Med Res. 2008 April:408-409.
Menon PR, Lodha R, Sivanandan S, Kabra SK. Intermittent or daily short course chemotherapy for tuberculosis in children: meta-analysis of randomized controlled trials. Indian Pediatr. 2010 Jan;47(1):67-73. Epub 2009 May 20.doi: https://doi.org/10.1007/s13312-010-0009-2.
Hong Kong Chest Service / British Medical Research Council. Controlled trial of 4 three-times-weekly regimens and a daily regimen all given for 6 months for pulmonary tuberculosis, Second report: The results up to 24months. Tubercle 1982;63:89-98.doi: https://doi.org/10.1016/s0041-3879(82)80044-5.
Subramani R, Santha T, Frieden TR, Radhakrishna S, Gopi PG, Selvakumar N, Sadacharam K, et al. Active Community surveillance of the impact of different tuberculosis Control measure, Tiruvallur, South India,1968-2001. Int. J. Epidemiol Advance Access, 2006:1-7.doi: https://doi.org/10.1093/ije/dyl216.
Philips S. A view of the overall problem, In: S. Philips(Ed) Current problems in tuberculosis. Springfield, Charles C Thomas Publ. 1966:109-15.
Deshmukh PA, Shaw T. Pulmonary tuberculosis and diabetes mellitus. Ind J Tub 1984;31:114.
Tripathy SR, Kar KP, Chakraborthy DC, Majumdar AK. Diabetes mellitus and pulmonary tuberculosis – A prospective study. Ind J Tub 1984;31:122.http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.553.3931&rep=rep1&type=pdf.
Patel JC. Complications in 8793 cases of diabetes mellitus, 14 years study in Bombay Hospital, Bombay, India. Ind J Med Sci 1989;43:177.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative