
A comparative study of weight loss and co morbidity benefits between Laparoscopic Sleeve Gastrectomy and Laparoscopic Gastric Imbrication/Plication in morbid obesity
Abstract
Background: Laparoscopic sleeve gastrectomy (LSG) involves resection of a portion of the greater curvature of stomach. Laparoscopic greater curvature plication /imbrication (LGCP) involves plicating/imbricating the greater curvature without gastric resection.
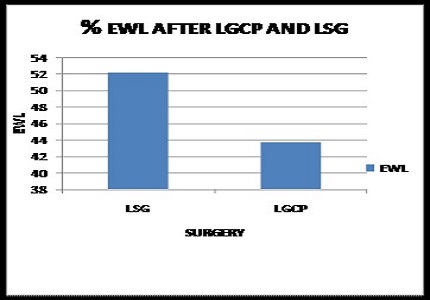
Materials and Methods: 30 patients who fulfilled the NIH criteria were randomized for either LSG (n = 15) [12 women and 3 men; mean age 38. 3 years (28–50 years) and mean BMI 43 kg/m2 or LGCP (n = 15) [10 women and 5 men; mean age 36.8 years (19–48years) and mean BMI 41 kg/m2. Patients were studied in terms of postoperative weight loss, changes in hypertension (systolic and diastolic blood pressure), FBS level and total cholesterol level. Follow-up period was 6 months. The mean hospital stay was 4 days for both groups. There were no intraoperative complications. All patients experienced postoperative excess weight loss and improvement in co morbid conditions. The improvement was significantly better in the LSG group in terms of excess weight loss (52.2% in LSG and 43.7% in LGCP) and change in FBS and Hypertension was not statistically significant (t test).
Conclusion: LGCP is feasible, safe, and effective, but has an inferior weight-loss effect as compared to LSG for morbidly obese patients with BMI above 40 kg/m2 and 35kg/m2 with co morbid conditions.
Downloads
References
2. Tsigos C, Hainer V, Basdevant A, Finer N, Fried M, Mathus-Vliegen E, Micic D, Maislos M, Roman G, Schutz Y, Toplak H, Zahorska-Markiewicz B; Obesity Management Task Force of the European Association for the Study of Obesity. Management of obesity in adults: European clinical practice guidelines. Obes Facts. 2008; 1(2):106-16. Doi: 10.1159/000126822. Epub 2008 Apr 18.
3. Blackburn GL, Walker WA. Science-based solutions to obesity: what are the roles of academia, government, industry, and health care? Am J Clin Nutr. 2005 Jul; 82(1 Suppl):207S-210S. [PubMed]
4. Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004 Oct 13; 292(14):1724-37. [PubMed]
5. DeMaria EJ. Bariatric surgery for morbid obesity. N Engl J Med. 2007 May 24; 356(21):2176-83. [PubMed]
6. Gumbs AA, Gagner M, Dakin G, Pomp A. Sleeve gastrectomy for morbid obesity. Obes Surg. 2007 Jul; 17(7):962-9. [PubMed]
7. Deitel M, Crosby RD, Gagner M. The First International Consensus Summit for Sleeve Gastrectomy (SG), New York City, October 25-27, 2007. Obes Surg. 2008 May; 18(5):487-96. Doi: 10.1007/s11695-008-9471-5. [PubMed]
8. Wilkinson LH, Peloso OA. Gastric (reservoir) reduction for morbid obesity. Arch Surg. 1981 May; 116(5):602-5. [PubMed]
9. M. Talebpour and B. S. Amoli, Laparoscopic total gastric vertical plication in morbid obesity. Journal of Laparoendoscopic and Advanced Surgical Techniques, vol. 17, no. 6, 1 Dec 2007 pp. 793–798,2007.
10. Gastrointestinal surgery for severe obesity. National Institutes of Health Consensus Development Conference Statement. Am J Clin Nutr 1992; 55(2 Suppl):615S–619S.
11. Silecchia G, Boru C, Pecchia A, Rizzello M, Casella G, Leonetti F, Basso N. Effectiveness of laparoscopic sleeve gastrectomy (first stage of biliopancreatic diversion with duodenal switch) on co-morbidities in super-obese high-risk patients. Obes Surg. 2006 Sep; 16(9):1138-44.
12. Mohamed M. Abouzeid, Osama Taha. Laparoscopic sleeve gastrectomy versus laparoscopic gastric greater curvature plication: a prospective randomized comparative study The Egyptian Journal of Surgery 2015, Vol 34; Issue 1; pp: 41–47.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative