
LARGE VESSEL VASCULITIS IN A CASE OF HLAB27 ASSOCIATED AXIAL SPONDYLOARTHRITIS
Abstract
A 24yr old male, with history of inflammatory back pain of 6 years, diagnosed as Radiographic axial spondyloarthritis, using alternate therapies, presented with incidentally found discrepancy of pulses and blood pressure in upper and lower extremities on follow up. Spondyloarthritis disease burden was high with elevated inflammatory markers, high disease activity was observed.
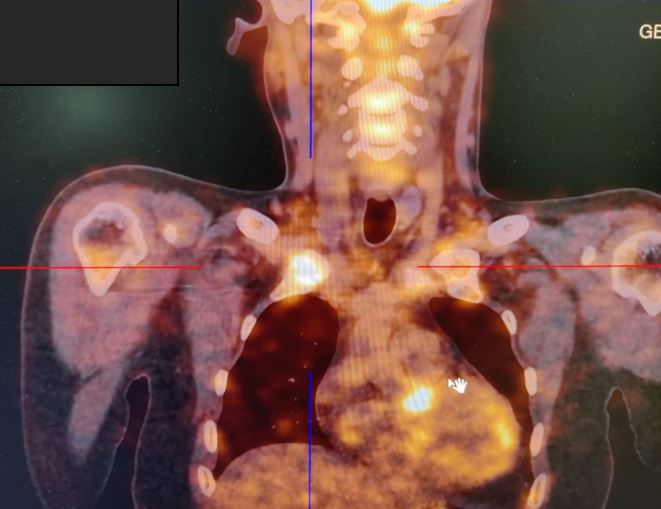
Imaging of blood vessels with CT aortography revealed thrombotic occlusion of upper limb arteries and stenosis of large vessels. Evaluation for underlying procoagulant state was negative. FDG- PET CT scan revealed metabolically active vasculitis involving ascending, arch, and descending aorta, brachiocephalic trunks with occlusive thrombosis of carotid and upper limb vessels. Concomitant occurrence of Takayasu arteritis with Ankylosing Spondylitis was contemplated, considering several reported associations of the two disorders in literature. But owing to the chronic underlying Axial Spondylitis with high disease activity, Spondyloarthritis associated aortitis was considered. High dose glucocorticoids were administered, Anti TNF agents initiated after latent TB prophylaxis.
Presence of high inflammatory markers in Spondyloarthritis should alert one to look for extra musculoskeletal manifestations in Spondyloarthritides in the form of vasculitis.
Downloads
References
2. KHAN MA. ANKYLOSING SPONDYLITIS : CLINICAL FEATURES. In: ANKYLOSING SPONDYLITIS: CLINICAL FEATURES. 2nd ed. 1998.
3. Sy A, Khalidi N, Dehghan N, Barra L, Carette S, Cuthbertson D, et al. Vasculitis in patients with inflammatory bowel diseases: A study of 32 patients and systematic review of the literature. Semin Arthritis Rheum. 2016;45(4).
4. Palazzi C, Salvarani C, D’Angelo S, Olivieri I. Aortitis and periaortitis in ankylosing spondylitis. Vol. 78, Joint Bone Spine. 2011.
5. Gan FY, Fei YY, Li MT, Wang Q, Xu D, Hou Y, et al. The characteristics of patients having ankylosing spondylitis associated with Takayasu’s arteritis. Clin Rheumatol. 2014;33(3).
6. Palazzi C, D’Angelo S, Lubrano E, Olivieri I. Aortic involvement in ankylosing spondylitis. Vol. 26, Clinical and Experimental Rheumatology. 2008.
7. Rivière E, Arnaud L, Ebbo M, Allanore Y, Claudepierre P, Dernis E, et al. Takayasu arteritis and spondyloarthritis: Coincidence or association? A study of 14 cases. Journal of Rheumatology. 2017;44(7).
Copyright (c) 2024 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative