
The sensitivity of electrodiagnostic criteria in subtype identification at the presentation in patients of Guillain-Barre syndrome
Abstract
Introduction: Electrophysiology plays a pivotal role in identifying various GBS subtypes. Despite having many electrodiagnostic criteria,studies addressing their applicability in patients of GBS at diagnosis are quite a few.
Purpose: This study evaluates the sensitivity of 5 known electrophysiological criteria in patients with GBS at the time of presentation.
Material & Methods: Clinical and electrophysiological data of GBS patients admitted with us between January 2011 and December 2016 were collected retrospectively from our hospital database, compiled and analyzed. For each patient, 5 different criteria for the electrophysiological diagnosis of GBS were applied, and the sensitivity of these 5 criteria in the diagnosis was evaluated.
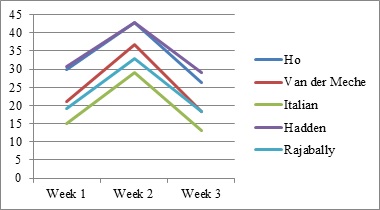
Results: A total of 288 patients were included. Closer concordance was noted between the criteria in diagnosing axonal subtype (Range- 36.81% to 41.32%).Italian criteria had the highest sensitivity (41.32%). There was a wider variation in the diagnosis of AIDP (Range- 19.79 to 34.72%). Hadden criteria showed the highest sensitivity (34.72%) closely followed by Ho et al (34.02%).
Conclusion: As the timing of Nerve Conduction Studies (NCS) and the severity of disease influence the grouping of each patient into a specific electrophysiologic subtype, one should be cautious in interpreting electrodiagnosticdata. Serial nerve conduction studies may be required to subtype each patient as electrophysiology evolves over the first few weeks of illness.
Downloads
References
Alter M. The epidemiology of Guillain-Barre! syndrome. Ann Neurol. 1990;27(S1):S7-S12. doi: https://doi.org/10.1002/ana.410270704.
Kleyweg RP, van der Meché FG, Schmitz PI. Interobserver agreement in the assessment of muscle strength and functional abilities in Guillain-Barré syndrome. Muscle Nerve. 1991;14(11):1103-1109.doi: https://doi.org/10.1002/mus.880141111.
Yadegari S, Kazemi N, Nafissi S. Clinical and electrophysiological features of Guillain-Barré syndrome in Iran. J ClinNeurosci. 2014;21(9):1554-1557. doi: https://doi.org/10.1016/j.jocn.2013.11.041.
Hughes RA, Cornblath, DR. Guillain-Barre syndrome. Lancet. 2005;366(9497):1653-1666. doi: https://doi.org/10.1016/s0140-6736(05)67665-9.
Blum S, Reddel S, Spies J, McCombe P. Clinical features of patients with Guillain-Barré syndrome at seven hospitals on the East Coast of Australia. J PeripherNervSyst. 2013;18(4):316-320. doi: https://doi.org/10.1111/jns5.12045.
Asbury AK, Arnason BG, Adams RD. The inflammatory lesion in idiopathic polyneuritis: Its role in pathogenesis. Medicine (Baltimore). 1969;48(3):173-215. doi: https://doi.org/10.1097/00005792-196905000-00001.
Hafer‐Macko CE, Sheikh KA, Li CY, Ho TW, Cornblath DR, McKhann GM, et al. Immune attack on the Schwann cell surface in acute inflammatory demyelinating polyneuropathy. Ann Neurol. 1996;39(5):625-635. doi: https://doi.org/10.1002/ana.410390512.
Kieseier BC, Kiefer R, Gold R, Hemmer B, Willison HJ, Hartung HP. Advances in understanding and treatment of immune-mediated disorders of the peripheral nervous system. Muscle Nerve. 2004;30(2):131-156. doi: https://doi.org/10.1002/mus.20076.
Yuki N. Pathogenesis of axonal Guillain–Barré syndrome: hypothesis. Muscle Nerve. 1994;17(6):680-682. doi: https://doi.org/10.1002/mus.880170619.
Asbury AK, Arnason BG, Karp HR, McFarlin DE. Criteria for the diagnosis of Guillain–Barré syndrome. Ann Neurol. 1978;15(3):565-566. doi: https://doi.org/10.1177%2F088307380001500308.
Albers JW, Donofrio PD, McGonagle TK. Sequential electrodiagnostic abnormalities in acute inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve. 1985;8(6):528-539. doi: https://doi.org/10.1002/mus.880080609.
Cornblath DR. Electrophysiology in Guillain–Barré syndrome. Ann Neurol. 1990;27:S517–S520. doi: https://doi.org/10.1002/ana.410270706.
Ho TW, Mishu B, Li CY, Gao CY, Cornblath DR, Griffin JW, Asbury AK, Blaser MJ, McKhann. GM: Guillain–Barre ´ syndrome in northern China. Relationship to Campylobacter jejuni infection and anti-glycolipid antibodies. Brain. 1995;118(3):597–605.
Visser LH, van der Meche FG, van Doorn PA, Meulstee J, Jacobs BC, Oomes PG, et al. Guillain– Barre syndrome without sensory loss (acute motor neuropathy). A subgroup with specific clinical, electrodiagnostic and laboratory features. Dutch Guillain–Barre Study Group. Brain. 1995;118(4):841–847.
Italian Guillain–Barre´ Study Group: The prognosis and main prognostic indicators of Guillain–Barre ´ syndrome. Brain. 1996;119(6):2053–2061.
Hadden RD, Cornblath DR, Hughes RA, Zielasek J, Hartung HP, Toyka KV, et al. Electrophysiological classification of Guillain-Barré syndrome: clinical associations and outcome. Plasma Exchange/SandoglobulinGuillain-Barré Syndrome Trial Group. Ann Neurol. 1998;44(5):780-788.
https://doi.org/10.1002/ana.410440512.
Rajabally YA, Hiew FL, Winer JB. Influence of timing on electrodiagnosis of Guillain-Barré syndrome in the first six weeks: a retrospective study. J Neurol Sci. 2015;357(1-2):143-145. doi: https://doi.org/10.1016/j.jns.2015.07.018.
Uncini A, Ippoliti L, Shahrizaila N, Sekiguchi Y, Kuwabara S. Optimizing the electrodiagnostic accuracy in Guillain-Barré syndrome subtypes: Criteria sets and sparse linear discriminant analysis. ClinNeurophysiol. 2017;128(7):1176-1183. doi: https://doi.org/10.1016/j.clinph.2017.03.048.
Alam TA, Chaudhry V, Cornblath DR. Electrophysiological studies in the Guillain-Barré syndrome: distinguishing subtypes by published criteria. Muscle Nerve. 1998;21(10):1275-1279. doi: https://doi.org/10.1002/(sici)1097-4598(199810)21:10%3C1275::aid-mus5%3E3.0.co;2-8.
Kalita J, Misra UK, Das M. Neurophysiological criteria in the diagnosis of different clinical types of Guillain-Barre syndrome. J NeurolNeurosurg Psychiatry. 2008;79(3):289-293. doi: https://doi.org/10.1136/jnnp.2007.118000.
Alexander M, Prabhakar AT, Aaron S, Thomas M, Mathew V, Patil AK. Utility of neurophysiological criteria in Guillain Barre΄ syndrome: subtype spectrum from a tertiary referral hospital in India. Neurol India. 2011;59(5):722-726. doi: https://doi.org/10.4103/0028-3886.86548
Hughes RA, Newsom-Davis JM, Perkin GD, Pierce JM. Controlled trial of prednisolone in acute neuropathy. Lancet. 1978;2(8093):750-753. doi: https://doi.org/10.1016/s0140-6736(78)92644-2.
De la O-Peña D, Robles-Figueroa M, Chávez-Peña Q, Bedolla-Barajas M. Features of Guillain-Barre syndrome in adults: results of a university hospital. Rev Med Inst Mex SeguroSoc. 2015;53(6):678-685.
Hahn AF. Guillain-Barré syndrome. Lancet 1998; 352(9128):635-641. doi: https://doi.org/10.1016/s0140-6736(97)12308-x.
Scarpino M, Lolli F, Carrai R, Lanzo G, Spalletti M, Barilaro A, et al. Diagnostic accuracy of neurophysiological criteria for early diagnosis of AIDP: A prospective study. Neurophysiol. Clin. 2016;46(1):35-42. doi: https://doi.org/10.1016/j.neucli.2015.12.008.
Copyright (c) 2020 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative