
From allergy to labial abscess following a bee sting: A Case report
Abstract
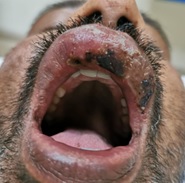
Arthropod bites are a common problem worldwide that are capable of inflicting injury, inciting allergic reactions, and transmitting systemic disease. Members of the Hymenoptera order in particular are of importance as they are nearly ubiquitous in nature and few such as bees, are also used for commercial purposes. These insects have stinging apparatus that deliver venom to the affected tissues during a bite. Hymenopteran venoms contain a mixture of proteins, peptides, and small organic molecules that produce varied effects. Stings from bees, wasps, and ants produce a wide array of clinical manifestations that can be local or systemic. Additionally, these stings may cause life-threatening allergic reactions. Anaphylaxis following a Hymenoptera sting is the most common serious systemic complication. Local reactions can be immediate or delayed. In a few instances, local or disseminated infections have also been reported following bee stings; although very rarely have proved fatal in severe cases. Infection rates are found to be higher in immunodeficiency states. Infections at site of a bee sting can result in the localized pustular lesion with peripheral induration or in severe cases deep necrotizing fascia infection with sepsis and multisystem organ failure. Here we report a case of a bee sting in the upper lip leading to the painful swelling with abscess formation successfully treated with antibiotics, incision, and drainage. Numerous mechanisms for infection in arthropod stings have been described; in our case report, we would like to highlight the importance of timely identification and appropriate management of the infections that may have a significant impact on the overall outcome.
Downloads
References
Dongol Y, Dhananjaya B L, Shrestha R K., Aryal G. Wasp venom toxins as a potential therapeutic agent. Protein Pept Lett. 2016;23(8):688-698. doi: https://doi.org/10.2174/0929866523666160511151039.
Ellis AK, Day JH. Clinical reactivity to insect stings. Curr Opin Allergy Clin Immunol. 2005;5(4):349-354. doi: https://doi.org/10.1097/01.all.0000174159.55756.58.
Sharmila RR, Chetan G, Narayanan P, Srinivasan S. Multiple organ dysfunction syndrome following single wasp sting. Indian J Peadiatr. 2007;74(12):57-58. doi: https://doi.org/10.1007/s12098-007-0208-6.
Junghanss T, Bodio M. Medically important venomous animals: biology, prevention, first aid, and clinical management. Clin Infect Dis. 2006;43(10):1309-1317. doi: https://doi.org/10.1086/508279.
Kim JH, Kim M, Lee SJ, Han SB, Hyon JY. Corneal bee sting controlled with early surgical intervention and systemic high-dose steroid therapy. Case Rep Ophthalmol Med. 2014. doi: https://doi.org/10.1155/2014/140626.
Alemán Navas RM, Mendoza MG M, Herrera H, de Herrera HP. Floor of the nose mucosa lysis and labial abscess caused by a bee sting. Braz Dent J. 2009;20(3):249-253. doi: https://doi.org/10.1590/s0103-64402009000300014.
David BK, Golden MD. Insect sting anaphylaxis. Immunol Allergy Clin North Am. 2007;27(2):261-268. doi: https://doi.org/10.1016/j.iac.2007.03.008.
Fernandez J, Soriano V, Mayorga L, Mayor M. Natural history of Hymenoptera venom allergy in Eastern Spain. Clin Exp Allergy. 2005;35(2):179-185. doi: https://doi.org/10.1111/j.1365-2222.2005.02169.x.
Steen CJ, Janniger CK, Schutzer SE, Schwartz RA. Insect sting reactions to bees, wasps, and ants. Int J Dermatol. 2005;44(2):91-94. doi: https://doi.org/10.1111/j.1365-4632.2005.02391.x.
Alexander MT, James DD, Grover MH. Fatal Infection after a Bee Sting. Clin Infect Dis. 2001;32(2):36-38. doi: https://doi.org/10.1086/318451.
Truskinovsky AM, Dick JD, Hutchins GM. Fatal infection after a bee sting. Clin Infect Dis. 2001;32(2):36-38. doi: https://doi.org/10.1086/318451.
Sherman RA. What physicians should know about africanizad honeybees. West J Med. 1995;163(6):541-546.
Klug R, Immerman R, Giron JA. Bee bite and the toxic shock syndrome. Ann Intern Med. 1982;96(3):382. doi: https://doi.org/10.7326/0003-4819-96-3-382_1.
Derlet RW, Richards JR. Cellulitis from Insect Bites: A Case Series. West J Emerg Med: Integ Emerg Care Population Health. 2003;4(2). Retrieved from https://escholarship.org/uc/item/45k424gt.
Copyright (c) 2020 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative