
Clinico-radiological profile and outcome of patients undergoing intercostal tube drainage in a tertiary care hospital in West Bengal, India
Abstract
Introduction: Evacuation of empyema which was first performed centuries ago, marked the beginning of thoracic drainage. The subsequent acquisition of a greater knowledge of the anatomy, physiology, and pathology of the pleural space directed the design of thoracic catheters and drainage systems and the development of the methods by which they are used. Thoracic drainage systems are designed to remove air and liquids from the pleural space or mediastinum, which collect there as a result of injury, disease, or surgical procedures.
Method: A total of 100 patients who underwent intercostal tube drainage due to various etiologies are followed up for 3 months in the study
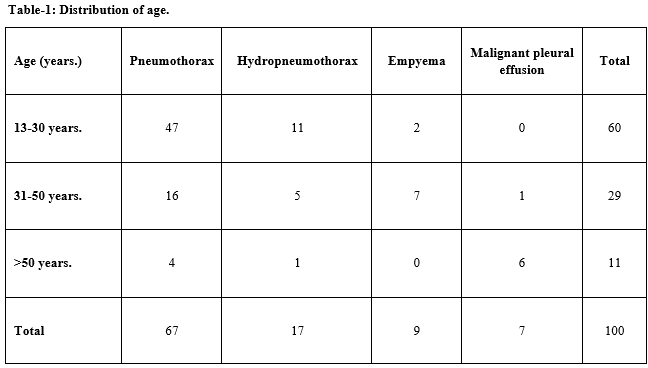
Results: In this study it was observed that pneumothorax (67%) as the most common indication for chest drain insertion followed by hydro-pneumothorax. During this period 100 patients of different pathologies related to chest underwent chest intubations. Amongst them 88(88%) were male and 12(12%) were female. Subcutaneous emphysema was found to be the most common complication followed by ICD tube blockage. Among the study population 95% patients were successfully treated & unsuccessful outcome was only 5%.
Conclusion: Chest tube insertion is a common procedure usually done for the purpose of draining accumulated air or fluid in the pleural cavity. Small-bore chest tubes (≤14F) are generally recommended as the first-line therapy for spontaneous pneumothorax in non-ventilated patients and pleural effusions in general. Large-bore chest drains may be useful for very large air leaks, as well as post-ineffective trial with small-bore drains.
Downloads
References
Emergency Nurses Association. Trauma nursing core course (Instructor Supplement). 5th ed 2000; ‘p.63-72, 278-282.
Emergency Nurses Association. Course in advanced trauma nursing-II: A conceptual approach to injury and illness (Student Manual), 2nd ed, 2003; p. 39-59.
Ganong, WF. Review of medical physiology. New York, NY: McGraw Hill Medical Publishing Division. 20th ed., 2001; p 644-673
Kapit, W., & Elson, LM. Anatomy coloring book, (). New York, NY: HarperCollins Publishers. 2nd ed, 2003; p. 91-97
Marino, PL. The ICU book. Baltimore, PA: Williams & Wilkins. 2nd ed. 1998; p. 459-62
Parsons, PE., & Heffner, JE. Pulmonary/Respiratory therapy secrets. Philadelphia, PA: Hanley & Belfus, Inc. 2nd ed, 2002; p. 68-73
Millikan J, Moore E, Steiner E, Aragon GE, Van Way CW 3rd. Complications of tube thoracostomy for acute trauma. Am J Surg 1980;140(6): 738-741. doi: https://doi.org/10.1016/0002-9610(80)90107-5.
Collop NA, Kim S, Sahn SA. Analysis of tube thoracostomy performed by pulmonologists at a teaching hospital. Chest 1997;112(3):709-713. doi: https://doi.org/10.1378/chest.112.3.709.
Aylwin CJ, Brohi K, Davies GD, Walsh MS. Prehospital and In- Hospital Thoracostomy: Indications and complications. Ann R Coll Surg Eng. 2008; 90(1):54-57. doi: https://doi.org/10.1308/003588408X242286.
Miller KS, Sahn SA. Review. Chest tubes. Indications, technique, management and complications. Chest. 1987;91(2):258-264. doi: https://doi.org/10.1378/chest.91.2.258.
Dural K, Gulbahar G, Kocer B, Sakinci U. A novel and safe technique in closed tube thoracostomy. J Cardiothorac Surg. 2010;5:21. doi: https://doi.org/10.1186/1749-8090-5-21.
Maritz D, Wallis L, Hardcastle T. Complications of tube thoracostomy for chest trauma. S Afr Med J. 2009; 99(2):114-117.
Bailey RC. Complications of tube thoracostomy in trauma. J Accid Emerg Med 2000; 17(2):111-114. doi: http://dx.doi.org/10.1136/emj.17.2.111.
Etoch SW, Bar-Natan MF, Miller FB, et al. Tube thoracostomy—factors related to complications. Arch Surg
;130(5):521-526. doi: https://dx.doi.org/10.1001/archsurg.1995.01430050071012.
Stark D, Federle M, Goodman P. CT and radiographic assessment of tube thoracostomy. AJR 1983;141(2): 253-258. doi: https://dx.doi.org/10.2214/ajr.141.2.253.
Omar HR, Abdelmalak H, Mangar D, Rashad R, Helal E, Camporesi EM. Occult pneumothorax,revisited. J Trauma Manag Outcomes. 2010; 4:12. doi: https://doi.org/10.1186/1752-2897-4-12.
Baldt M, Bankier A, Germann P, Poschl GP, Skrbensky GT, Herold CJ. Complications after emergency tube thoracostomy: assessment with CT. Radiol. 1995;195(2):539-543. doi: https://doi.org/10.1148/radiology.195.2.7724780.
Al- Tarshihi MI, Khamash FA, Al-Ibrahim AEO. Thoracostomy complications and pitfalls: An experience at tertiary care military hospital. Rawal Med J. 2008;33(2):141-144.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative