
Retrospective analysis of chest x-ray of patients from eastern Uttar Pradeshpresenting in Radiology department ofHind Institute Medical Sciences, Barabanki Uttar Pradesh
Abstract
Introduction: Chest Xray is one of the most frequently asked radiological examination in patients with heart or lung problems in general medical practice. There are many studies on correlation of CXR findings and other tools of investigations like CT scan, MRI and laboratory investigations like spirometry and sputum examinations etc. The present study aims at establishing a possible correlation in rural population of Eastern Uttar Pradesh.
Methods: We have done a cross sectional study in a period of six months including 2500 patients coming for CXR. Patients were followed up to a point where radiological diagnosis was confirmed or otherwise after other investigations and clinical response.
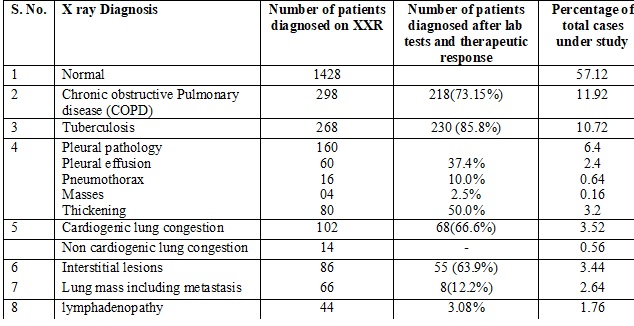
Results: There was fairly good correlation in patients with COPD (73.15%), tuberculosis (85.8%), interstitial lung disease (63.9%) and congestive heart failure (68.6%).
Conclusion: We conclude that CXR is tool of reasonable sensitivity however there is sizeable possibility of false positive and negative cases.
Downloads
References
Chakraborty AK. Epidemiology of tuberculosis: current status in India. Indian J Med Res. 2004 Oct;120(4):248-76.
Jindal SK. Emergence of chronic obstructive pulmonary disease as an epidemic in India. Indian J Med Res. 2006 Dec;124(6):619-30.
Chhabra SK, Chhabra P, Rajpal S, et al. Ambient air pollution and chronic respiratory morbidity in Delhi. Arch Environ Health. 2001 Jan-Feb;56(1):58-64.
Behera D, Kashyap S. Pattern of malignancy in a north Indian hospital. J Indian Med Assoc. 1988 Feb;86(2):28-9.
Karai GS, Nath HK, Paul G, et al. Carcinoma of the lung. A record and analysis of 100 cases. Indian J Cancer. 1967 Jun;4(2):105-13.
Dasgupta A, Bagchi A, Nag S, et al. Profile of respiratory problems in patients presenting to a referral pulmonary clinic. Lung India. 2008 Jan;25(1):4-7. doi: http://www.lungindia.com/text.asp?2008/25/1/4/44129.
Karen L Lipkind, M Ed. Division of healthcare statistics. Advanced data, Number 276, June 10, 1996, NCHS From Vital and Health Statistics of the center for Control and prevention.
Chhabra SK, Kumar R, Gupta U, et al. Prediction equations for spirometry in adults from northern India. Indian J Chest Dis Allied Sci. 2014 Oct-Dec;56(4):221-9.
Rajpal,S, Dhingra. and Aggarwal. Sputum grading as predictor of treatment outcome in pulmonary tuberculosis., Ind.J.Tub.,2002,49:139-41.
Gruber P, Swadron, S. DeBlieux, P. and Nelson, B. The acute Presentation of Chronic Obstructive pulmonary Diseases in the Emergency Department: A Challenging Oxymoron. Emergency Medicine Practice 2008:10, 11:1-27.
BTS COPD Consortium (2005). Spirometry in practice – a practical guide to using spirometry in primary care. British Thoracic Society, London Pp 8–9
Pudney, E. and Doherty, M. Plain chest x-ray (CXR) in the diagnosis of chronic obstructive pulmonary disease (COPD)” European Respiratory J. 2016:48,60:DOI: 10.1183/13993003.
Chugh, T, Goel,N. and Kumar. Physiological and radiological correlation in COPD. Ind. J. Chest Dis. And Allied Sci. 2012,54:235-242.
Policy Recommendations for smoking cessation and treatment of tobacco dependence. World Health Organization Tobacco Free initiative 2008.:. Pp 15–40.
Jindal SK. Emergence of chronic obstructive pulmonary disease as an epidemic in India. Indian J Med Res. 2006 Dec;124(6):619-30.
Horne,D.J. Royce, S.E.,Gooze,L Narita,M., Hopewell, P.M., Nahid, P& Steingart,K.R.”Sputum Monitoring during Tuberculosis Treatment for Predicting Outcome: A Systematic Review and Meta-analysis”Lancet Infect Dis. 2010 10(6): 387–394.
World Health organization: Definitions and reporting framework for tuberculosis: 2013 revision, Geneva, WHO. Accessed 2016.
van Cleeff MR, Kivihya-Ndugga LE, Meme H, et al. The role and performance of chest X-ray for the diagnosis of tuberculosis: a cost-effectiveness analysis in Nairobi, Kenya. BMC Infect Dis. 2005 Dec 12;5:111.
Attili AK, Kazerooni EA, Gross BH, et al. Smoking-related interstitial lung disease: radiologic-clinical-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1383-96; discussion 1396-8. doi: https://doi.org/10.1148/rg.285075223.
Bradley S, Abraham S., Grice A., López P.R,, Wright J., Farragher, T. Shinkins B and Neal, R.D. Sensitivity of chest X-ray for lung cancer: systematic review. Br J Gen Pract 2018; 68,1
Moon,J.N. “Diagnostic tools of pleural effusion”Tuberc Respir Dis (Seoul). 2014 May; 76(5): 199–210.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative