A Case Report on Treatment of Pancreatoblastoma in a 55-year-old female with acute pancreatitis
Priyanka1*, Hemanth Vudayaraju2, V. Sai Sindhuja3
DOI:https://doi.org/10.17511/ijmrr.2025.i02.09
1* Priyanka, MS (General Surgery), DNB (General Surgery), DrNB (Surgical Oncology), FALS (Oncology), Yashoda Hospitals, Secunderabad, Telangana, India.
2 Hemanth Vudayaraju, MS (General Surgery), MCh (Surgical Oncology), DNB (Surgical Oncology), Director-Surgical Oncology and Minimal Access Onco Surgery and Robotic Surgeon, Yashoda Hospitals, Secunderabad, Telangana, India.
3 V. Sai Sindhuja, MS (General Surgery), Resident DrNB (Surgical Oncology), Yashoda Hospitals, Secunderabad, Telangana, India.
Background: Pancreatoblastoma is a rare, malignant tumor that develops in the pancreas and is distinguished by lobular structures which contain acinar cells and squamoid corpuscles. The most common site was the head of the pancreas, and the most common symptom is abdominal pain and vomiting.
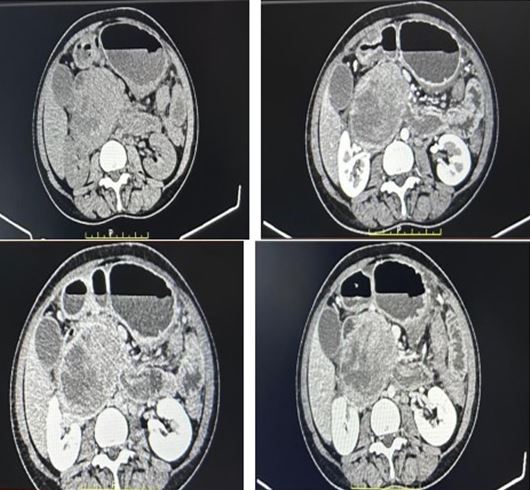
Case Presentation: A 55-year-old female presented with complaints of abdominal pain and vomitings with vitals in normal range. However, her serum amylase and lipase levels were found to be elevated. A contrast-enhanced computed tomography (CECT) revealed a large exophytic mass lesion in her pancreas, measuring 6.5 x 9.3 x 8.5 cm and causing distortion of the SMV medially and stretching of the anterior superior pancreaticoduodenal vein. The main pancreatic duct is severely compressed. Our patient underwent a Whipple procedure and exhibited an unremarkable recovery.
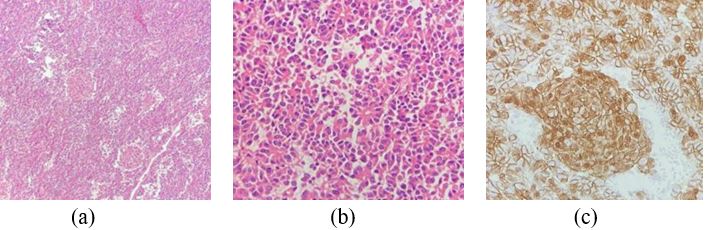
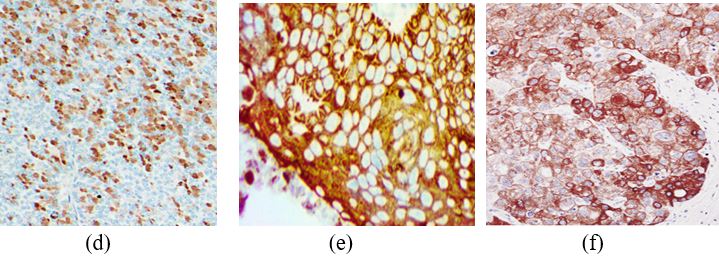
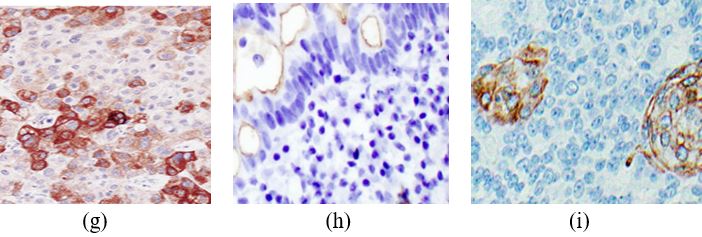
Conclusion: Pancreatoblastoma is a curable tumor that requires early diagnosis through a multi-disciplinary approach. The tumor is removed completely by surgery and pathology; Immunohistochemistry confirms the diagnosis. Following surgery, the patient is closely monitored to look for any residual disease, metastases, or recurrences.
Keywords: Pancreatoblastoma, amylase, lipase, Whipple procedure, immuno-histochemistry
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MS (General Surgery), DNB (General Surgery), DrNB (Surgical Oncology), FALS (Oncology), , Yashoda Hospitals, Secunderabad, Telangana, India. Email:  |
Priyanka, Hemanth Vudayaraju, V. Sai Sindhuja, A Case Report on Treatment of Pancreatoblastoma in a 55-year-old female with acute pancreatitis. Int J Med Res Rev. 2025;13(2):41-45. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1552 |
 |
 ©
©