Correlation Between Impulse Oscillometry and Spirometry in Assessment Of Small Airway Dysfunction In Asymptomatic Smokers
Harishankar S1*, Sreekala C2, Fathahudeen A3
DOI:https://doi.org/10.17511/ijmrr.2025.i01.05
1* Harishankar S, Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
2 Sreekala C, Associate Professor, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
3 Fathahudeen A, Professor and Head of the Department, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
Background: The traditional pulmonary function tests may be inadequate to detect Chronic Obstructive Pulmonary Disease (COPD) pathological damage and smoking-related lung disease. An impulse oscillation system (IOS) is a novel method for reactance and airway resistance measurements. It is a kind of forced oscillation, where sound waves oscillate at different frequencies, usually between 5 and 20 Hz, and propagate through the bronchial tree. It measures the proximal airway resistance (measured at 20 Hz [R20]), the peripheral airway resistance (measured at R5–R20), and the overall airway resistance (measured at 5 Hz [R5]). Resistance and reactance make up impedance. IOS provides more detailed information than spirometry on regional lung function and should be considered as being complementary to spirometry to comprehensively assess lung function in COPD.
Objectives: The objective of our study is to assess the correlation between impulse oscillometry and spirometry parameters in small airway dysfunction in asymptomatic smokers in a tertiary care centre; and to determine the association of smoking index with impulse oscillometry small airway dysfunction parameter R5-R20.
Materials And Methods: The study was conducted in the Department of Pulmonary Medicine, Medical College Hospital, Thiruvananthapuram. The present cross-sectional study included asymptomatic current smokers, eligible participants underwent spirometry and oscillometry and the results were compared.
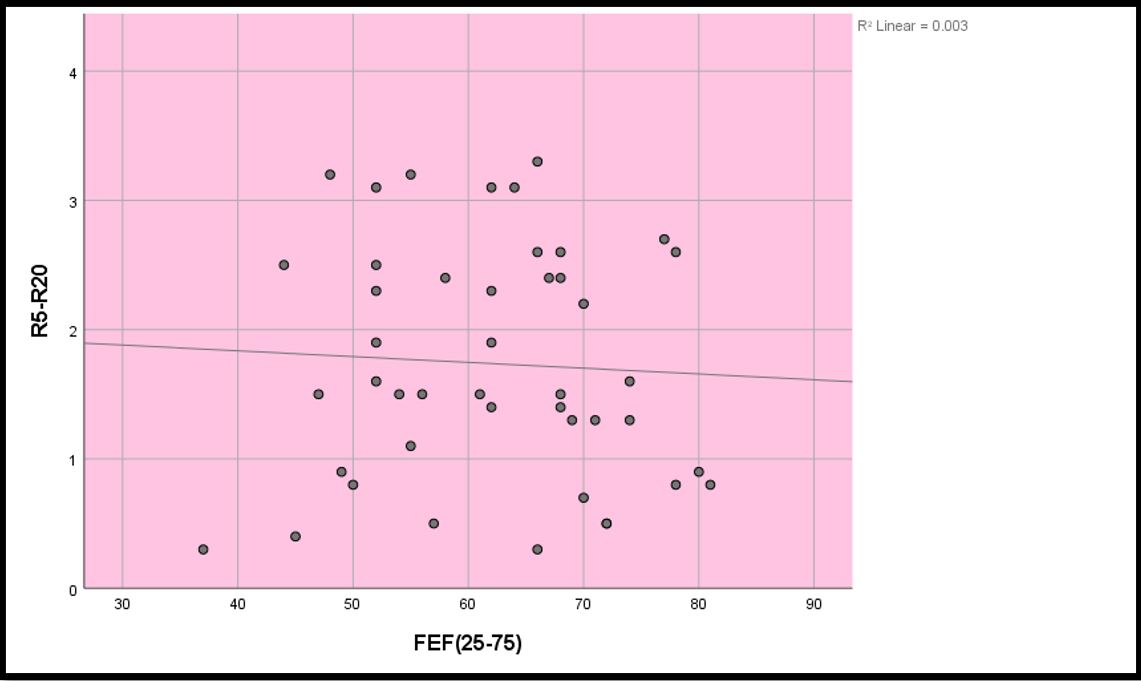
Results: Out of 45 patients studied, 44.4% (n=20), fell within the 45-60 age range. The majority of participants, comprising 37.8% (n=17), had a Smoking Index ranging from 300 to 399. Correlation analysis between FEF (25-75) vs (R5-R20) done by Pearson correlation test reported a very mild negative correlation between them (r=-0.053, p=0.728). The chi-square test reported a significant association between smoking index & R5-R20 (p<0.05).
Conclusion: Impulse oscillometry is capable of detecting SAD in asymptomatic smokers with preserved spirometry and with FEF(25-75) values in the normal range. We verify that IOS offers parameters that can contribute to conventional pulmonary function tests.
Keywords: Forced oscillation technique, spirometry, resistance, reactance, small airway dysfunction, impulse oscillometry, forced expiratory flow (25–75%), smoking index
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India. Email:  |
Harishankar S, Sreekala C, Fathahudeen A, Correlation Between Impulse Oscillometry and Spirometry in Assessment Of Small Airway Dysfunction In Asymptomatic Smokers. Int J Med Res Rev. 2025;13(1):26-32. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1518 |
 |
 ©
© 
 = 41
= 41