Prevalence of Anti Thyroid Peroxidase Antibody Positivity in Subclinical and Clinical Hypothyroidism subjects attending a tertiary centre in South India
Anil Kumar R1*, Lalitha R2, Surekha B Shetty3
DOI:https://doi.org/10.17511/ijmrr .2024.i04.03
1* R Anil Kumar, Professor and HOD, Karnataka Institute of Endocrinology and Research, Bengaluru, Karnataka, India.
2 R Lalitha, Professor, Karnataka Institute of Endocrinology and Research, Bangalore, Karnataka, India.
3 Surekha B Shetty, Professor, Karnataka Institute of Endocrinology and Research, Bangalore, Karnataka, India.
Objective: To estimate the prevalence of anti-TPO antibodies in subjects with subclinical and clinical hypothyroidism in subjects attending a tertiary centre in South India.
Materials and Methods: 50 subjects with subclinical hypothyroidism and 120 subjects with clinical hypothyroidism attending the out-patient department of Karnataka Institute of Endocrinology and Research, Bangalore were included over one year from June 2023 to June 2024. Weight, height, and waist circumference measurements were obtained using standardised techniques. Fasting plasma glucose, postprandial plasma glucose, HBA1c, and lipid profile, of these subjects were determined. TSH, FT4 and anti-TPO antibodies were estimated by chemiluminescent immunoassay.
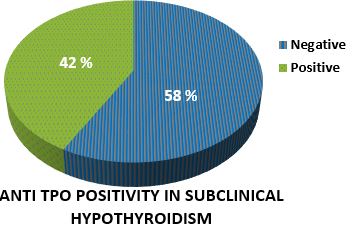
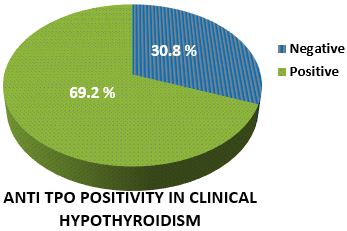
Results: 170 subjects with hypothyroidism were studied. Out of 50 subjects with subclinical hypothyroidism,64% were females. 70% of patients had a BMI of more than 25. Waist circumference was greater than 80 cm in 96% of patients. A family history of hypothyroidism was present in 16%. Anti-TPO antibody was positive in 42% of the subjects. Total cholesterol, LDL and triglyceride levels were higher in anti-TPO-positive subjects. Out of 120 subjects with clinical hypothyroidism,76.7% were females. 74.9% of patients had a BMI of more than 25. Waist circumference was more than 80 cms in 92% of patients. A family history of hypothyroidism was present in 24.2% of the subjects. Anti-TPO antibody was positive in 69.2% of the subjects. Total cholesterol, LDL and triglyceride levels were higher in anti-TPO-positive patients.
Conclusions: Prevalence of anti-TPO antibody was present in 42% of subclinical hypothyroidism patients. As anti-TPO positive patients progress to clinical hypothyroidism at a higher rate than negative patients, estimation of anti-TPO antibodies should be an integral part of an investigation of subclinical hypothyroidism. Prevalence of anti-TPO antibody was present in 69.2% of clinical hypothyroidism patients.
Keywords: Anti-thyroid peroxidase antibodies, Hypothyroidism, TSH
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor and HOD, , Karnataka Institute of Endocrinology and Research, Bengaluru, Karnataka, India. Email:  |
Anil Kumar R, Lalitha R, Surekha B Shetty, Prevalence of Anti Thyroid Peroxidase Antibody Positivity in Subclinical and Clinical Hypothyroidism subjects attending a tertiary centre in South India. Int J Med Res Rev. 2024;12(4):109-110. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1488 |
 |
 ©
©