Influence of Family History on the Age of Onset and Complication Spectrum in Patients with Type 2 Diabetes Mellitus
Innanje Vidhya1*, Ganagarajan Inbaraj2, Raghavendra Rao Mohan3
DOI:https://doi.org/10.17511/ijmrr .2024.i04.02
1* Innanje Vidhya, Assistant Professor, Department of Diabetology, Karnataka Institute of Endocrinology and Research, Bengaluru, Karnataka, India.
2 Ganagarajan Inbaraj, Department of Neurology, National Institute of Mental Health and Neurosciences, Bangalore, Karnataka, India.
3 Raghavendra Rao Mohan, Director, Central Council for Research in Yoga Naturopathy, New Delhi, India.
Type 2 Diabetes Mellitus (T2DM) is a prevalent chronic health condition globally, with its onset and complications significantly influenced by genetic and environmental factors. This study aimed to assess the influence of family history on the age of onset and complication spectrum among T2DM patients.
Methods: This descriptive cross-sectional study recruited 500 participants diagnosed with T2DM. Data were collected through structured interviews and clinical assessments, focusing on demographics, medical and family history, age of onset, and diabetes-related complications. Chi-square and logistic regression analyses were employed to examine the association between family history and diabetes complications, adjusting for confounders.
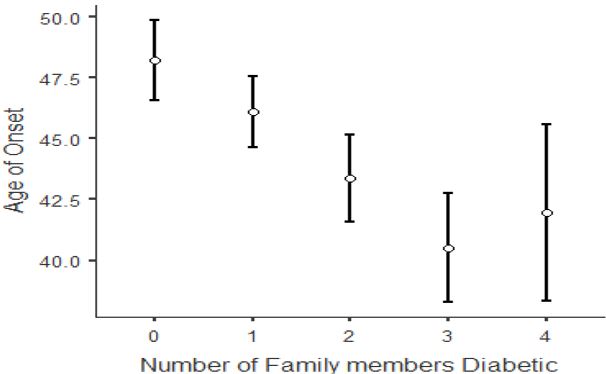
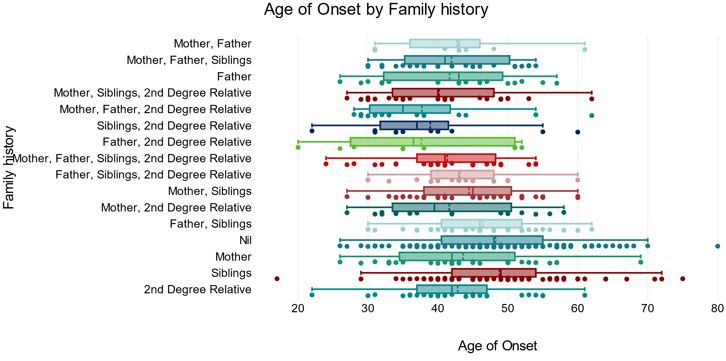
Results: Among the participants, 73.8% reported a positive family history. The mean age of onset for those with a family history was significantly lower (43.8 ± 9.86 years) compared to those without (48.24 ± 9.87 years; p < 0.001). Patients with higher HbA1c levels were younger, had an earlier onset of diabetes, and a higher prevalence of hypertension. The age of onset was earlier, if more family members had a history of diabetes. Complications were present in 80.8% of the cohort, with the most common being diabetic peripheral neuropathy (70.6%). Logistic regression analysis indicated that having siblings with diabetes was a significant predictor for general diabetic complications (OR=2.589, CI: 1.481 to 4.53, p<.001), diabetic retinopathy (OR=1.981, CI: 1.20 to 3.26, p=0.007), and diabetic peripheral neuropathy (DPN) (OR=1.709, CI: 1.042 to 2.8, p=0.034).
Conclusion: The study highlights the significant influence of family history on the age of onset and the spectrum of complications in T2DM. These findings suggest the necessity for comprehensive family history assessments in clinical settings to identify at-risk individuals for early intervention and personalized management strategies.
Keywords: Type 2 Diabetes Mellitus, family history, age of onset, diabetes-related complications, cross-sectional study
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Diabetology, Karnataka Institute of Endocrinology and Research, Bengaluru, Karnataka, India. Email:  |
Innanje Vidhya, Ganagarajan Inbaraj, Raghavendra Rao Mohan, Influence of Family History on the Age of Onset and Complication Spectrum in Patients with Type 2 Diabetes Mellitus. Int J Med Res Rev. 2024;12(4):99-108. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1487 |
 |
 ©
©