Differences Between Premenopausal And Postmenopausal Coronary Artery Disease (CAD) Risk Factors and Clinical Profile
MS H1*, Bhuiyan M2, Sowdagar M3, Siddique N4, Paul G5, Paul P6, Shakil S7, Khan M8, Sohan A9, Alam M10, Hoque M11
DOI:https://doi.org/10.17511/ijmrr .2024.i04.04
1* Hossain MS, Assistant Professor, Department Of Cardiology, Mymensingh Medical College Mymensingh Bangladesh, Bangladesh.
2 MAS Bhuiyan, Assistant Professor, Department Of Cardiology, Mymensingh Medical College Mymensingh, Bangladesh.
3 MNH Sowdagar, Associate Professor and Head, Department Of Cardiology, Border Guard Hospital Dhaka, Bangladesh.
4 NA Siddique, Assistant Professor, Department of Cardiology, Mymensingh Medical College Mymensingh, Bangladesh.
5 GK Paul, Associate Professor and Head, Department Of Cardiology, Mymensingh Medical College Mymensingh, Bangladesh.
6 PK Paul, Consultant, Department Of Cardiology, Mymensingh Medical College Hospital Mymensingh, Bangladesh.
7 SS Shakil, Senior Consultant, Department of Cardiology, Mymensingh Medical College Hospital Mymensingh, Bangladesh.
8 MTI Khan, Registrar, Department Of Cardiology, Mymensingh Medical College Hospital Mymensingh, Bangladesh.
9 AM Sohan, Associate Professor, Department Of Cardiology, Ahsania Medical College Uttara Dhaka, Bangladesh.
10 MM Alam, Associate Professor, Department of Cardiology, Dhaka National Medical College Dhaka, Bangladesh.
11 MS Hoque, Consultant, Department Of Cardiology, BSMMU Dhaka, Bangladesh.
Introduction: Coronary artery disease is the leading cause of mortality and morbidity of both men and women accounting for over one-third of total deaths. It has reached epidemic proportions among Indians. It accounts for 1 out of 3 womens deaths regardless of race or ethnicity. In women, the annual mortality rate from CAD is high.
Methods: A prospective observation study was conducted at the cardiology department, NICVD, Dhaka, Bangladesh from January to December 2019. A total of 200 female CAD patients were drawn from the cardiology department. A total of 50 premenopausal cases and 150 postmenopausal cases were enrolled according to their status at the time of diagnosis. All patients underwent percutaneous coronary intervention and were given conventional drug therapy for coronary artery disease during follow-up.
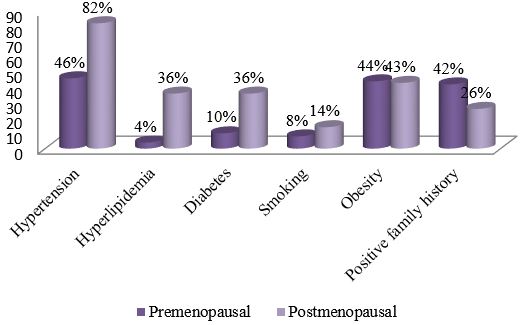
Results: Differences were compared between the 2 groups. Fewer premenopausal women suffered from hypertension (46% versus 82%, P< 0.001), type 2 diabetes (10% versus 36%, P = 0.001), and hyperlipidemia (4% versus 36%, P<0.001), but more had a positive family history of premature CAD (42% versus 26%, P = 0.03). The cumulative recurrence rate was 1.76 times higher in postmenopausal patients than in premenopausal patients. Clinical diagnosis (HR = 2.54, 95%CI: 1.21-4.85, P = 0.02) and type 2 diabetes (HR = 4.10, 95%CI: 2.37-8.83, P = 0.004) were two factors that influenced recurrence in premenopausal subjects, while the clinical diagnosis (HR = 1.93, 95%CI: 1.59-3.46, P = 0.03) and Gensini score (HR =1.20, 95% CI: 1.11-1.45, P = 0.02) were influencing factors in the postmenopausal patients.
Conclusion: Our study clarified the differences between postmenopausal and premenopausal women concerning risk factors, clinical symptoms, cardiovascular features, and recurrence rate, and provided a reference for further study on the mechanism and prognosis in postmenopausal or premenopausal CAD patients.
Keywords: Premenopausal, Postmenopausal, Coronary Artery Disease (CAD), Risk Factors
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department Of Cardiology, Mymensingh Medical College Mymensingh Bangladesh, , , Bangladesh. Email:  |
MS H, Bhuiyan M, Sowdagar M, Siddique N, Paul G, Paul P, Shakil S, Khan M, Sohan A, Alam M, Hoque M, Differences Between Premenopausal And Postmenopausal Coronary Artery Disease (CAD) Risk Factors and Clinical Profile. Int J Med Res Rev. 2024;12(4):116-117. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1477 |
 |
 ©
©