Expert opinion on the clinical approach of using sodium glucose cotransporter-2 inhibitors for managing diabetic patients with cardiovascular and renal complications in Indian settings
Manjula S1*, Krishna Kumar M2
DOI:https://doi.org/10.17511/ijmrr.2024.i01.03
1* Manjula S, Sr Vice President, Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India.
2 Krishna Kumar M, Sr General Manager, Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India.
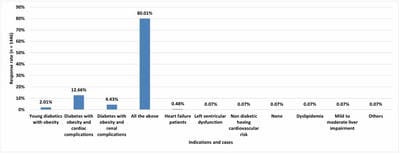
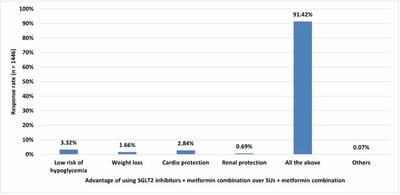
Objective: To evaluate the prescription practice of sodium-glucose co-transporter-2 (SGLT2) inhibitors with a special focus on dapagliflozin to treat cardiac and renal disorders in obese Indian diabetic patients. Methods: A cross-sectional, questionnaire-based study was conducted to collect the perspectives of physicians with expertise in treating diabetic obese patients with cardiac and renal disorders in endocrinology across India between June 2022 and December 2022. Descriptive statistics were used to summarize the characteristics of the study by employing frequencies and percentages. Results: Among the 1,446 survey participants, 80% of them indicated that young diabetic patients with obesity, and obese patients with cardio-renal complications may require SGLT2 inhibitors. Furthermore, patients aged between 41-50 and 51-60 years also required SGLT2 inhibitors for diabetes management according to 57% and 27% of the respondents. The majority of the respondents (91.29% and 90.53%) recommended dapagliflozin as the best SGLT2 inhibitor for treating patients with chronic kidney disease and heart failure. Additionally, about 59% and 66% of the experts indicated that patients would experience an average weight loss of 2-3 kilograms and an average blood pressure reduction of 3-6 mm Hg after 12 weeks of treatment with dapagliflozin, respectively. Conclusion: Experts recommend the use of SGLT2 inhibitors for the treatment of young diabetic patients with obesity and obese subjects with cardiorenal complications. Dapagliflozin monotherapy was preferred for patients with chronic kidney disease and heart failure. Furthermore, experts highly recommend the combinations of dapagliflozin + metformin and DPP4 inhibitors + metformin + dapagliflozin for effective diabetes management.
Keywords: Chronic kidney disease, Diabetes, Dapagliflozin, Heart failure, Obesity
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Sr Vice President, Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India. Email:  |
Manjula S, Krishna Kumar M. Expert opinion on the clinical approach of using sodium glucose cotransporter-2 inhibitors for managing diabetic patients with cardiovascular and renal complications in Indian settings. Int J Med Res Rev. 2024;12(1):22-28. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1457 |
 |
 ©
©