The general skeletal features of Multicentric Carpotarsal Osteolysis: what the radiologist needs to know
Albahkali S1*, Alsaiady M2
DOI: https://doi.org/10.17511/ijmrr.2023.i06.03
1* Salha M Albahkali, Resident, Radiology Department, King Saud Medical City, Riyadh, Saudi Arabia.
2 Moath Alsaiady, Pediatric Radiology Consultant, Radiology Department, King Saud Medical City, Riyadh, Saudi Arabia.
Purpose of review: Radiographic imaging is the first investigational step in detecting Multicentric carporarsal osteolysis, and the radiologist must be aware then familiar with the radiological features in order both to reach a prompt diagnosis and then to classify the patient’s condition at this important time for considering early management. Here we review the literature on this topic. Recent Findings: Patients with multicentric carpotarsal osteolysis (MCTO) are frequently diagnosed with juvenile idiopathic arthritis (JIA). Initially, their symptoms are arthritic and include pain, swelling and stiffness. Among the many published studies, some are case reports that describe the phenotypical manifestations with a brief discussion of the radiographic findings and subsequently of the genetic analysis which eventually leads to a definitive diagnosis. Some patients develop end-stage renal failure, and a delay in identifying this condition can lead to unfavorable progression of the disease. In addition, we found reports of joint inflammation based on imaging and pain relief with antirheumatics for osteolysis and bone destruction. Various studies discuss the radiological findings, including the disappearance of the carpal and tarsal bones. Others describe the genetic mutations, including MAFB, that are associated with the condition, and its possible management through the use of therapeutic drugs. A very recent description of serial radiographs taken from a young age suggests that dysfunctional bone formation can play a role in the skeletal phenotype of MCTO. Summary: The unique features of clinical presentation, atypical radiological findings, failure to obtain remission with medical treatment and consanguinity, should guide clinicians towards the diagnosis of this condition. We summarize the X-ray findings which are highly specific and can therefore differentiate with confidence between this condition and others. Further performance of gene.
Keywords: Multicentric carpo-tarsal osteolysis, Skeleton, MAFB, Nephropathy, Radiologist.
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Radiology Department, King Saud Medical City, Riyadh, , Saudi Arabia. Email:  |
Albahkali S, Alsaiady M, The general skeletal features of Multicentric Carpotarsal Osteolysis: what the radiologist needs to know. Int J Med Res Rev. 2023;11(6):146-158. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1454 |
 |
 ©
©  Figure 1: Nine-year-old presenting with skeletal deformity and renal osteodystrophy:
Figure 1: Nine-year-old presenting with skeletal deformity and renal osteodystrophy: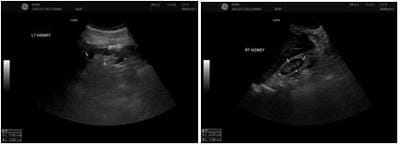 Figure 2: 9 years old girl presnted with ESRD, renal ultrasound Findings.
Figure 2: 9 years old girl presnted with ESRD, renal ultrasound Findings. Figure 3. Nine-year-old girl presenting with ESRD, radiological X-ray findings:
Figure 3. Nine-year-old girl presenting with ESRD, radiological X-ray findings: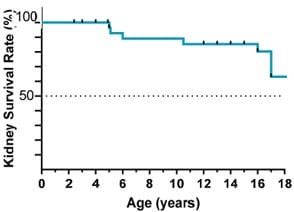 Figure 4: Kidney failure-free survival until adulthood.
Figure 4: Kidney failure-free survival until adulthood.


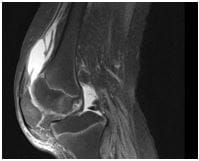 Figure 8: Nine-year-old known case of end stage renal disease on automated peritoneal dialysis, presenting with left knee swelling:
Figure 8: Nine-year-old known case of end stage renal disease on automated peritoneal dialysis, presenting with left knee swelling: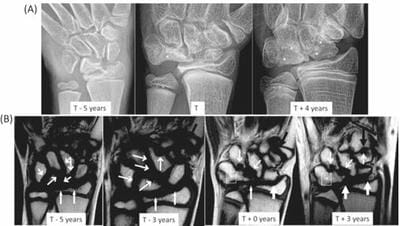
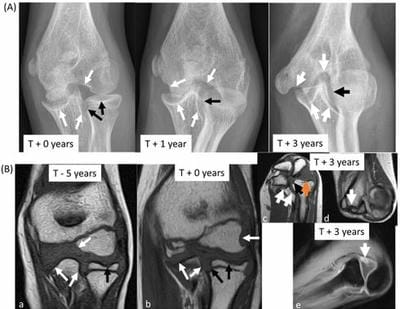 Figure 10: Images of the left elbow. (A). The left elbow's frontal radiographs show several progressive erosions in the ulna, humerus, and radius (black and white arrows, respectively), along with a progressive deformity of the distal humerus and overgrowth of the subluxed radial head. (B) (a,b,c,d) T1 signal-weighted MR images of the left elbow show several progressive erosions in the coronal plane (a, b) of the radius and ulna (orange arrows) and humerus (blue arrows). By 2020, acquisition in standard planes was impossible for the patient due to a fixed flexion deformity (c, d). (e) Radio-capitellar subluxation and synovitis (arrow) are visible in the post-contrast T1 signal-weighted image with fat saturation.
Figure 10: Images of the left elbow. (A). The left elbow's frontal radiographs show several progressive erosions in the ulna, humerus, and radius (black and white arrows, respectively), along with a progressive deformity of the distal humerus and overgrowth of the subluxed radial head. (B) (a,b,c,d) T1 signal-weighted MR images of the left elbow show several progressive erosions in the coronal plane (a, b) of the radius and ulna (orange arrows) and humerus (blue arrows). By 2020, acquisition in standard planes was impossible for the patient due to a fixed flexion deformity (c, d). (e) Radio-capitellar subluxation and synovitis (arrow) are visible in the post-contrast T1 signal-weighted image with fat saturation. Figure 11:
Figure 11:
 Figure 13: Joint inflammation on MRI. A, B: Presence of joint effusions and synovitis in bilateral ankle compartments at age 19 months. These images are prior to initiation of treatment with anti-rheumatic agents. C: Redemonstration of diffuse inflammation in bilateral wrists after discontinuation of methotrexate therapy (32).
Figure 13: Joint inflammation on MRI. A, B: Presence of joint effusions and synovitis in bilateral ankle compartments at age 19 months. These images are prior to initiation of treatment with anti-rheumatic agents. C: Redemonstration of diffuse inflammation in bilateral wrists after discontinuation of methotrexate therapy (32).