Dengue Serotypes In Manipur – Findings From A Retrospective Analytical Study In A Tertiary Care Hospital
Anand Singh L1, Suson T2*, Geeta Chanu C3, Ranjana Devi K4, Rebachandra Singh H5
DOI: https://doi.org/10.17511/ijmrr.2023.i06.02
1 Laitonjam Anand Singh, Scientist C Virus Research Diagnostic Laboratory VRDL, Department of Microbiology, Regional Institute of Medical Sciences, Imphal, Manipur, India.
2* Thingujam Suson, Scientist B Virus Research Diagnostic Laboratory VRDL, Department Of Microbiology, Regional Institute Of Medical Sciences, Imphal, Manipur, India.
3 Chongtham Geeta Chanu, Research Assistant Virus Research Diagnostic Laboratory VRDL, Department Of Microbiology, Regional Institute of Medical Sciences, Imphal, Manipur, India.
4 Khuraijam Ranjana Devi, Principal Investigator VRDL and Professor Head, Department Of Microbiology, Regional Institute of Medical Sciences, Imphal, Manipur, India.
5 Heigrujam Rebachandra Singh, CoPrincipal Investigator VRDL Professor, Department Of Microbiology, Regional Institute of Medical Sciences, Imphal, Manipur, India.
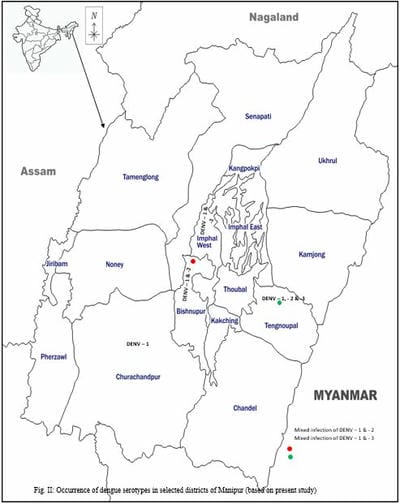
Objectives: As a part of an ongoing research programme on vector-borne viral diseases especially Dengue, a retrospective analytical study on the occurrence and distribution of Dengue virus serotype(s) in the state of Manipur – a small state situated in the northeastern region of the Indian subcontinent was carried out at Viral Research & Diagnostic Laboratory (VRDL), Department of Microbiology, Regional Institute of Medical Sciences (RIMS), Imphal which is a tertiary care hospital. Materials & Methods: A total of 914 blood samples from clinically dengue-suspected patients were screened for the presence of Dengue infection by adopting the ELISA (IgM) technique during the period from 01/06/2022 to 02/12/2022. Further, anti-Dengue IgM antibody-positive samples having high Optical Density (OD) value(s) were selected and subjected to RT PCR to determine the serotype(s) of the Dengue virus. Results: Of the 914 blood samples examined for the presence of Dengue infection, 111 (12.14%) were found positive for anti-Dengue IgM antibody indicating acute infection of Dengue virus. Of the positive patients, there were 56 (50.45%) males and 55 (49.54%) females. Predominant clinical features observed among the Dengue-confirmed patients included – fever (74%), headache (19%), arthralgia / joint pain (9%), myalgia (6%) and vomiting (6%) respectively. The study revealed that while the circulation of three (03) Dengue virus serotypes, namely DENV – 1, DENV – 2 & DENV – 3 were observed in the Tengnoupal district, the circulation of two Dengue virus serotypes i.e., DENV – 1 & DENV – 2 was evident in Imphal West & Bishnupur districts respectively. The present study also reveals the occurrence of Dengue virus serotype – 1 (DENV - 1) in Churachandpur district. Conclusion: The present study reveals the circulation/distribution of three Dengue virus serotypes namely, DENV – 1, DENV – 2 and DENV – 3 among the studied samples.
Keywords: Dengue virus, Dengue IgM ELISA, Dengue serotype (RT PCR)
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Scientist B Virus Research Diagnostic Laboratory VRDL, Department Of Microbiology, Regional Institute Of Medical Sciences, Imphal, Manipur, India. Email:  |
Anand Singh L, Suson T, Geeta Chanu C, Ranjana Devi K, Rebachandra Singh H, Dengue Serotypes In Manipur – Findings From A Retrospective Analytical Study In A Tertiary Care Hospital. Int J Med Res Rev. 2023;11(6):136-145. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1452 |
 |
 ©
© 
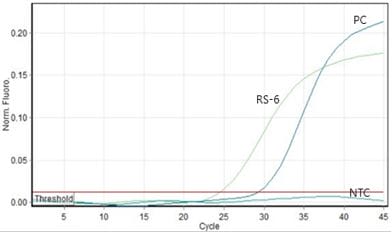
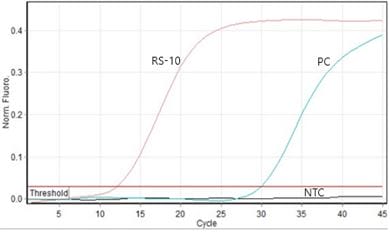
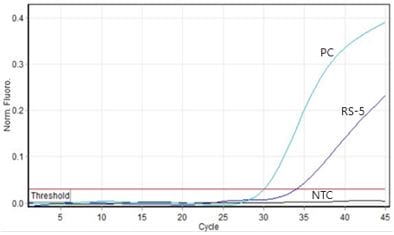 1(e): Amplification curve for RS-5
1(e): Amplification curve for RS-5