The Effect Of Umbilical Cord Milking In Reducing ROP Of Preterm Babies
Abdul Mannan M.1*, Akhter S.2, Tamima Nasrin U.3, Reza Ali T.4, Chowdhury N.5, Sharfuddin Ahmed M.6
DOI: https://doi.org/10.17511/ijmrr.2023.i04.02
1* Md. Abdul Mannan, Professor , Department of Neonatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
2 Shamima Akhter, Medical Officer, Upazilla Health Complex, Homna, Cumilla, Bangladesh.
3 Ummey Tamima Nasrin, Assistant Surgeon, Upazilla Health Complex, Chandina, Cumilla, Bangladesh.
4 Tariq Reza Ali, Associate Professor (Vitreo- Retina), Department of Ophthalmology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
5 Nuzhat Chowdhury, Professor (Vitreo- Retina), Department of Ophthalmology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
6 Md. Sharfuddin Ahmed, Professor and Ex Chairman, Department of Community Ophthalmology, BSMMU and Vice-Chancellor, BSMMU, Dhaka, Bangladesh.
Background: Recent advances in neonatal care in the last decade have improved the survival rates for premature infants. Consequently, the incidence of ROP has increased in parallel. Prematurity, low birth weight, respiratory distress syndrome, mechanical ventilation, prolonged oxygen treatment and blood transfusion increase the risk of ROP. Methodology: Neonates born before 37 weeks of gestation were assigned to either umbilical cord milking or non-milking group at a 1: 1 ratio according to a computer-generated randomized sequence. After delivery of a baby umbilical cord milking was performed by holding the infant at the level of the placenta. The first eye evaluation for ROP was done at 20 days of age for gestational age less than 30 weeks & weight below 1200gm & at 30 days of age for gestational age more than 30 weeks & above weight 1200gm. Follow-up was continued until retinal vascularization was completed. The follow-up schedules were organized depending on the retinal findings. The retinal finding was evaluated according to the International Classification of Retinopathy of Prematurity. The patients were grouped as no ROP, mild ROP (stages I-II ROP without plus disease, showed regression), and severe ROP (zone 1 or zone 2, stage III, aggressive ROP without stages, stage II with plus disease who required treatment). Results: 114 newborns were enrolled in this study. Then among 114 preterm neonates 57 were randomized to the umbilical cord milking group and 57 were randomized to no milking group. Baseline characteristics were almost similar between the two groups. There was a significant increase in hematocrit level 57.3 ±3.5 V 47.4 ± 4.5 (P value less than 0.001), reduction in need of blood transfusion 3.5% V 42.1% (P value less than 0.001) & reduction in ROP 3.5% V 19.3% (P 0.007). Conclusion: This study concluded that umbilical cord milking after delivery improves hematocrit levels, reduces the need for blood transfusion & reduces the incidence of ROP in preterm infants.
Keywords: Umbilical Cord Milking, Retinopathy of Prematurity, Preterm, Blood Transfusion, RCT
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor , Department of Neonatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, , Bangladesh. Email:  |
Md. Abdul Mannan, Shamima Akhter, Ummey Tamima Nasrin, Tariq Reza Ali, Nuzhat Chowdhury, Md. Sharfuddin Ahmed, The Effect Of Umbilical Cord Milking In Reducing ROP Of Preterm Babies. Int J Med Res Rev. 2023;11(4):89-95. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1439 |
 |
 ©
© 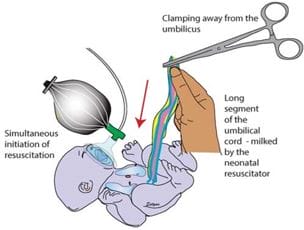 Figure 1: Umbilical cord milking.
Figure 1: Umbilical cord milking. Figure 2: Umbilical cord milking after delivery.
Figure 2: Umbilical cord milking after delivery.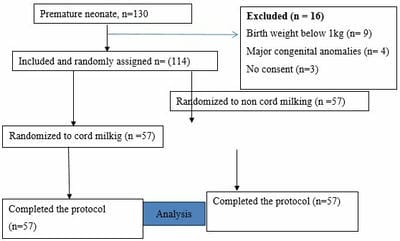 Figure-3: CONSORT flow diagram for study.
Figure-3: CONSORT flow diagram for study.