Study of the prognostic effect of diabetes in patients of pulmonary tuberculosis
Kumar S.1*, Kumar Jha D.2
DOI: https://doi.org/10.17511/ijmrr.2023.i03.02
1* Sushil Kumar, Assistant Professor, Department of Medicine, Mednirai Medical College, Palamu, Jharkhand, India.
2 Dharmendra Kumar Jha, Associate Professor and Head, Department of Medicine, Mednirai Medical College, Palamu, Jharkhand, India.
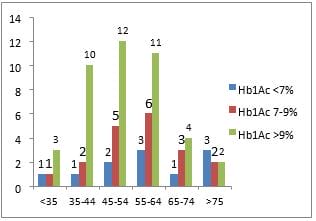
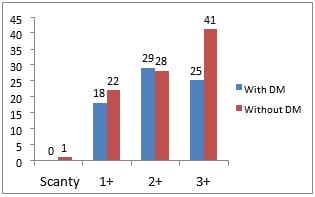
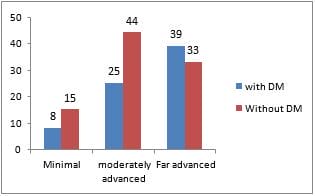
Background: There is a synergistic effect between diabetes mellitus and pulmonary tuberculosis. India has the highest number of tuberculosis patients and India has also the second-highest number of patients with diabetes mellitus in the world. The dual curse of these two diseases may have an impact on both sides as an outcome of treatment and poor glycaemic control. There were many studies have been done about the relationship between diabetes and tuberculosis but still there is a large gap about its synergistic effect. Methods: In this study, we include 164 patients with pulmonary tuberculosis aged more than 18 years 72 out of 164 patients are diabetic and 92 patients are nondiabetic. Demographic details, physical and clinical examination, Blood sugar fasting and postprandial, Hba1c, x-rays chest, sputum for AFB and CBNAAT test have been done on all patients then ATT was given to patients and appropriate antidiabetic treatment given to diabetic patients. follow up done on all patients on the 2nd month and 6th months. Results: In this study, the commonest age group for tuberculosis infection is 45-54 but in diabetic patients common age group for tuberculosis infection is 55-64. Patients of diabetes and tuberculosis commonly have elevated Hba1c and relatively poor treatment outcome reflected by a sputum conversion rate of 77.7%, 16.7%has failed treatment and also diabetic patients has 3+ sputum positivity. Conclusions: In patients with tuberculosis screening of diabetes may improve treatment outcomes and prevent complications by appropriate management of diabetes and tuberculosis.
Keywords: Tuberculosis, Diabetes mellitus, Coinfection, Hba1c, CBNAAT
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Medicine, Mednirai Medical College, Palamu, Jharkhand, India. Email:  |
Sushil Kumar, Dharmendra Kumar Jha, Study of the prognostic effect of diabetes in patients of pulmonary tuberculosis. Int J Med Res Rev. 2023;11(3):65-70. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1418 |
 |
 ©
©