Monitoring and Evaluation of Adverse Drug Reaction In Emergency Medicine Department: A Prospective Observational Study
N. Patel S.1*, M. Patel S.2, R. Patel K.3, S. Patel K.4
DOI: https://doi.org/10.17511/ijmrr.2023.i02.03
1* Shreya N. Patel, Tutor, Department of Pharmacology, NHL Municipal Medical College, Ahmedabad, Gujrat, India.
2 Sanskruti M. Patel, Final Year Undergraduate Student, NHL Municipal Medical College, Ahmedabad, Gujrat, India.
3 Kinal R. Patel, Final Year Undergraduate Student, NHL Municipal Medical College, Ahmedabad, Gujrat, India.
4 Krima S. Patel, Intern, NHL Municipal Medical College, Ahmedabad, Gujrat, India.
Background: Any deviation from the intended beneficial effect of medication results in a drug-related problem. Adverse drug reactions (ADRs) are negative consequences of drug therapy. It is the fourth to the sixth leading cause of mortality in the United States of America. Aims: To find out the proportion of medical emergency admissions that are secondary to Adverse Drug Reactions(ADRs). Settings and Designs: An observational, prospective study conducted at the Emergency Medicine Department, at Tertiary Care Teaching Hospital for 12 months, daily from 9 am to 5 pm. Materials and Methods: Patients aged ≥ 18, who have given written informed consent were included and patients not able to give willing consent and women presented with pregnancy were excluded from the study. The data was recorded in the case record form, The causality assessment was performed using the WHO causality assessment scale. To determine the ADR severity, the Modified Hartwig and Siegel scale was used. Statistical Analysis: The statistical evaluation was done with the help of Statistical Package for Social Science (SPSS) version 21.0 manufactured by IBM (demo version) and Microsoft Excel 2016. p< 0.05 was considered statistically significant. Results: Elderly patients were having a higher incidence of ADRs. Among all drug groups, the highest incidence was antimicrobials and drugs acting on blood. The majority of patients either recovered or were in a recovery phase. Most of the ADRs were not preventable. Conclusions: Reporting ADRs systematically allows appropriate analysis and intervention which will improve the patient’s safety. Many ADRs could be preventable by avoiding certain drug/drug combinations, hospitalization, dose-dependent side effects, appropriate individual dosing and applying for the Antimicrobial Stewardship Programme.
Keywords: Adverse Drug Reactions(ADRs), Antimicrobials, Emergency Medicine Department
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Tutor, Department of Pharmacology, NHL Municipal Medical College, Ahmedabad, Gujrat, India. Email:  |
Shreya N. Patel, Sanskruti M. Patel, Kinal R. Patel, Krima S. Patel, Monitoring and Evaluation of Adverse Drug Reaction In Emergency Medicine Department: A Prospective Observational Study. Int J Med Res Rev. 2023;11(2):41-47. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1413 |
 |
 ©
© 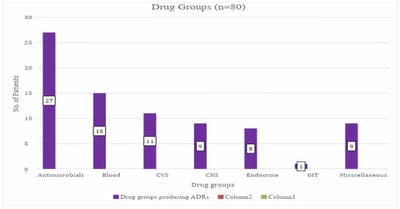 Figure 1: Drug groups of the ADRs.
Figure 1: Drug groups of the ADRs. 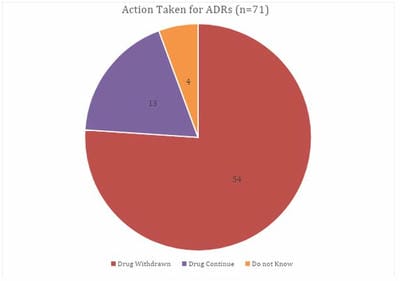 Figure 2: Action taken by a clinician for the ADRs.
Figure 2: Action taken by a clinician for the ADRs.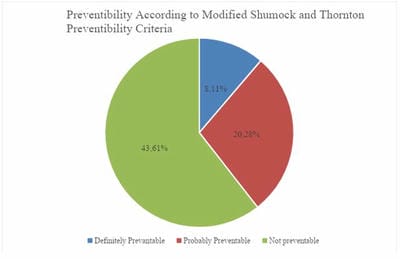 Figure: 3 Preventability of patients with ADRs according to Modified Schumock and Thornton Preventability Criteria
Figure: 3 Preventability of patients with ADRs according to Modified Schumock and Thornton Preventability Criteria 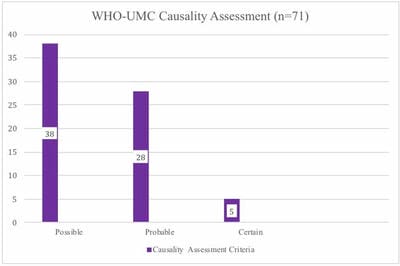 Figure: 4 Causality Assessment of the Adverse Drug Reactions (ADRs).
Figure: 4 Causality Assessment of the Adverse Drug Reactions (ADRs).