Lymph node metastasis after neoadjuvant chemotherapy
Dutta P.1*, Wadhawan G.2
DOI: https://doi.org/10.17511/ijmrr.2023.i01.03
1* Pooja Dutta, Post Graduate Resident, Department of General Surgery, Pacific Medical College and Hospital, Bhilon ka Bedla, Udaipur, Rajasthan, India.
2 Gaurav Wadhawan, Professor, Department of General Surgery, Pacific Medical College and Hospital, Bhilon ka Bedla, Udaipur, Rajasthan, India.
Neoadjuvant therapy refers to the systemic treatment of breast cancer prior to definitive surgical therapy (ie, preoperative therapy). Neoadjuvant chemotherapy is offered to patients with locally advanced breast cancer and also those breast cancer patients who may benefit from size reduction before conservation therapy. Response to neoadjuvant chemotherapy is evaluated by the change in tumor size from pretreatment clinical and/or radiologic measurement to post-treatment status. The spectrum of response to neoadjuvant chemotherapy varies from complete response, partial response, to non-response. This concept is the same in breast tumors as well as axillary lymph nodes. The presented case is a known case of Triple Negative Invasive Ductal carcinoma with Axillary involvement Right Breast since November, 2020 and had undergone Neoadjuvant Chemotherapy till February 2021, followed by surgical intervention in October 2022.
Keywords: Triple Negative Breast carcinoma, Axillary Lymph node metastasis, Neoadjuvant Chemotherapy, Defaulter
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Post Graduate Resident, Department of General Surgery, Pacific Medical College and Hospital, Bhilon ka Bedla, Udaipur, Rajasthan, India. Email:  |
Pooja Dutta, Gaurav Wadhawan, Lymph node metastasis after neoadjuvant chemotherapy. Int J Med Res Rev. 2023;11(1):18-21. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1411 |
 |
 ©
©  Figure 1
Figure 1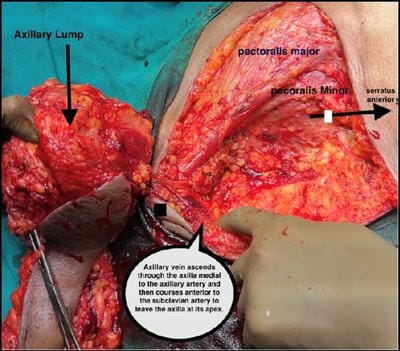 Figure 2
Figure 2 Figure 3
Figure 3