The window of opportunity in axial spondyloarthritis: A Stitch in Time
Ghosh P.1*, Kumar Sarma P.2, Shenoy P.3, Mukherjee D.4, Desai A.5
DOI: https://doi.org/10.17511/ijmrr.2022.i05.04
1* Parasar Ghosh, Professor and HOD, Department of Clinical Immunology and Rheumatology, Institute of Postgraduate Medical Education and Research and SSKM Hospital, Kolkata, West Bengal, India. https://orcid.org/0000-0001-9023-5169
2 Pradip Kumar Sarma, HOD, Department of Rheumatology and Clinical Immunology, Excel Care Hospital, Guwahati, Assam, India. https://orcid.org/0000-0003-2043-3682
3 Padmanabha Shenoy, Medical Director, Center For Arthritis and Rheumatism Excellence, Kerala, India. https://orcid.org/0000-0002-7666-1361
4 Dhrubojyoti Mukherjee, Senior Medical Scientific Liaison, Novartis Healthcare Private Limited, India. https://orcid.org/0000-0003-4104-4117
5 Akshay Desai, Franchise Medical Head, Novartis Healthcare Private Limited, India. https://orcid.org/0000-0001-7491-0558
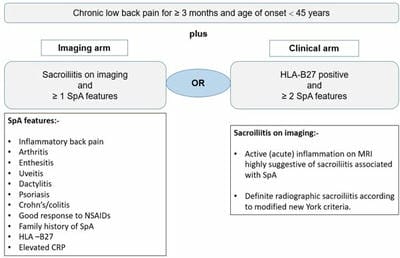
Axial spondyloarthritis comprising both non-radiographic axial spondyloarthritis and ankylosing spondylitis has a deleterious impact on the patient’s quality of life with a detrimental outcome of structural damage. Although in the current era of diagnostic advancements, axSpA can be diagnosed early within a short period after the onset of symptoms, but still there is a delay of up to several years in many parts of the world. The concept of a window of opportunity is primarily derived from rheumatoid arthritis, which is relevant in the context of axSpA based upon the early diagnosis and to commence highly effective treatment with biologics like anti-TNF and anti-IL-17 to modify the disease process for arresting structural damage or syndesmophytes formation. Still, challenges exist for early diagnosis of SpA in patients with low back pain which ultimately creates a barrier to effective treatment initiation. More robust researches along with the available evidence on both the aspects of clinical and imaging factors are the way forward for the early identification of susceptible individuals for early intervention with a better outcome.
Keywords: Ankylosing Spondylitis, Axial Spondyloarthritis, Non-Radiographic Axial Spondyloarthritis, Magnetic Resonance Imaging, Sacroiliac Joint, Sacroiliitis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor and HOD, Department of Clinical Immunology and Rheumatology, Institute of Postgraduate Medical Education and Research and SSKM Hospital, Kolkata, West Bengal, India. Email:  |
Parasar Ghosh, Pradip Kumar Sarma, Padmanabha Shenoy, Dhrubojyoti Mukherjee, Akshay Desai, The window of opportunity in axial spondyloarthritis: A Stitch in Time. Int J Med Res Rev. 2022;10(5):154-165. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1398 |
 |
 ©
©