New Onset of Diabetes in Adults with Post-Covid Infection in a Tertiary Care Hospital
Abburu A.1*, Aftab K.2, Priscilla I.3, Meruva K.4
DOI: https://doi.org/10.17511/ijmrr.2022.i04.02
1* Alekhya Abburu, Post Graduate Intern, Kamineni Academy of Medical Sciences and Research Centre, Hyderabad, Telangana, India.
2 Kainat Aftab, Post Graduate Intern, Kamineni Academy of Medical Sciences and Research Centre, Hyderabad, Telangana, India.
3 Irene Priscilla, Post Graduate Intern, Kamineni Academy of Medical Sciences and Research Centre, Hyderabad, Telangana, India.
4 Karthik Meruva, Assistant Professor, Department of General Medicine, Kamineni Academy of Medical Sciences and Research Centre, Hyderabad, Telangana, India.
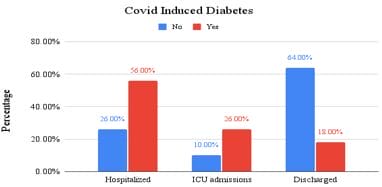
Aim/Scope: This study is aimed to investigate the incidence of diabetes after infection with the coronavirus (COVID-19). SARS COV2 is a rapidly spreading disease which causes morbidity and mortality. One of the most important complications associated with covid 19 is Diabetes Mellitus. Materials & Methods: This was a retrospective descriptive study of (50 diabetic and 50 non-diabetic) patients who had a previous history of covid-19 and who are infected during the second wave (Aug’21-Oct’21) at a tertiary care hospital, Hyderabad, India. Data collected including patient demographic and baseline characteristics like patient’s age, sex and history of covid infection were analyzed using Statistical Package for Social Sciences (SPSS) software version 22.0. Results: In the study among covid infected(n=50) subjects who were tested diabetic after Long Covid, 28(56%) were hospitalized, 13(26%) were found to have ICU admissions and 9(18%) were discharged with mild covid symptoms and the subjects(n=50) who didn’t have any symptoms of diabetes after Long Covid, majority 32(64%) were found to be discharged with mild covid symptoms, 5(10%) were found to have ICU admissions and 13 (26%)were found to be hospitalized with the critical covid condition. It was observed that patients hospitalized with critical covid conditions were susceptible to onset of diabetes (p-value: 0.10) Conclusion: This study showed a high incidence of complications in patients infected with COVID-19 with diabetes being the most common one. Patients with poor glycemic control should be routinely monitored and treated appropriately
Keywords: COVID 19, diabetes, HbA1c, SARS COV2
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Post Graduate Intern, , Kamineni Academy of Medical Sciences and Research Centre, Hyderabad, Telangana, India. Email:  |
Alekhya Abburu, Kainat Aftab, Irene Priscilla, Karthik Meruva, New Onset of Diabetes in Adults with Post-Covid Infection in a Tertiary Care Hospital. Int J Med Res Rev. 2022;10(4):122-127. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1392 |
 |
 ©
©