A Multi-centre Study to Evaluate the Long-Term Efficacy and Safety of Biosimilar Infliximab (Infimab™) in Ankylosing Spondylitis in Real-world Clinical Settings - A perspective from Eastern India
Kumar Sarma P.1*, Mukherjee S.2, Sarkar R.3, Kumar Mandal S.4, Patra P.5, Bose T.6, Surin A.7, Naorem S.8, Basu K.9, Parida J.10, Arunachalam C.11
DOI: https://doi.org/10.17511/ijmrr.2022.i04.01
1* Pradip Kumar Sarma, Consultant, Excel Care Hospital, Ring Road, Guwahati, Assam, India.
2 Sukumar Mukherjee, Consultant, GD Diabetes Institute, Lelin Sarani, Kolkata, West Bengal, India.
3 R N Sarkar, Consultant, GD Diabetes Institute, Lelin Sarani, Kolkata, West Bengal, India.
4 Santosh Kumar Mandal, Consultant, NH RNT Hospital, Mukundapur, Kolkata, West Bengal, India.
5 Pradeepta Patra, Professor, SUM Hospital, Nandan Kanan, Bhubaneswar, Odisha, India.
6 Tanoy Bose, Consultant, NH Surgical Institute, Hiland Park, Kolkata, West Bengal, India.
7 Ajit Surin, Professor, SUM Hospital, Nandan Kanan, Bhubaneswar, Odisha, India.
8 Santa Naorem, Professor, RIMS, Rims Road, Imphal, Imphal West, Manipur, India.
9 Kaushik Basu, Professor, Medical College Kolkata, 88 College Street, Kolkata, West Bengal, India.
10 J.R. Parida, Professor, SUM Hospital, Nandan Kanan, Bhubaneswar, Odisha, India.
11 CT Arunachalam, Senior Marketing Manager, Sun Pharma, Mumbai, Maharashtra, India.
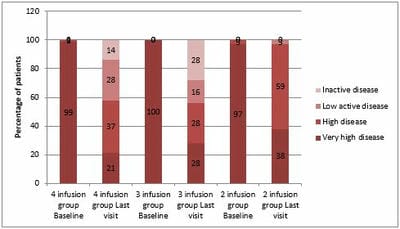
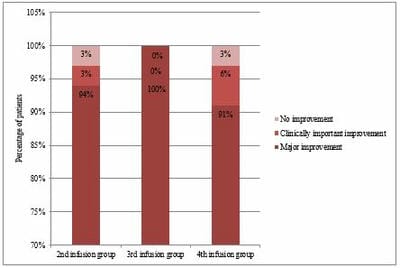
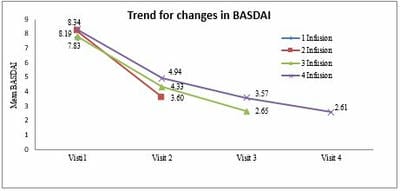
Introduction: Owing to dearth of data on infliximab biosimilars in Indian patients, a pan-India case database-based study with infliximab biosimilar BOW015 (Infimab™) was carried out to capture its efficacy and safety in real-world clinical settings in India. Here, we assessed its efficacy and safety in ankylosing spondylitis (AS) among patients in East India cohort. Materials and methods: Patients who were given BOW015 for other indications, prior innovator infliximab or other biologics were excluded from study. The primary variable was Ankylosing Spondylitis Disease Activity Scale (ASDAS) response defined as change of > 2 in ASDAS score from baseline by 4-6 months of follow-up. Results: The cohort consisted of 149 patients, predominantly male (69.8%), with a mean (±SD) age of 36.75 (±11.11) years and mean (±SD) body weight of 58.26 (±15.4) kgs. Of treated patients, 91 (61.1%) patients were administered four doses, 10 (6.7%) patients were administered three doses, 37 (24.8%) patients were administered two doses and 11 (7.4%) patients were administered only a single dose of BOW015. In final analysis set, 81 patients had data at baseline and 4th visit. Among 81 patients, 74 (91%) patients achieved major improvement, 5 (6%) patients achieved clinically important improvement and 2 (3%) were non-responders at 4th visit. Conclusion: Infimab™ (BOW015) showed significant improvement in ASDAS and BASDAI in patients with AS at end of 4-6 months of follow-up with its clinical benefits being apparent as early as first dose of BOW015.
Keywords: Biosimilar, Infliximab, Ankylosis Spondylitis, ASDAS, BASDAI, Real-World
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant, , Excel Care Hospital, Ring Road, Guwahati, Assam, India. Email:  |
Pradip Kumar Sarma, Sukumar Mukherjee, R N Sarkar, Santosh Kumar Mandal, Pradeepta Patra, Tanoy Bose, Ajit Surin, Santa Naorem, Kaushik Basu, J.R. Parida, CT Arunachalam, A Multi-centre Study to Evaluate the Long-Term Efficacy and Safety of Biosimilar Infliximab (Infimab™) in Ankylosing Spondylitis in Real-world Clinical Settings - A perspective from Eastern India. Int J Med Res Rev. 2022;10(4):113-121. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1390 |
 |
 ©
© 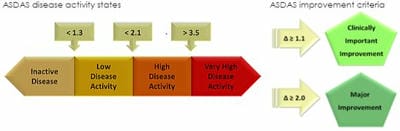 Figure 1: Categorization based on ASDAS
Figure 1: Categorization based on ASDAS Figure 2: Flow chart of AS patients treated with biosimilar Infliximab (BOW015)
Figure 2: Flow chart of AS patients treated with biosimilar Infliximab (BOW015)