Quality Improvement Project in the introduction of Major Trauma and Major Haemorrhage Protocol
Chowdhury D.1*
DOI: https://doi.org/10.17511/ijmrr.2022.i03.03
1* Debkumar Chowdhury, Specialist Registrar, Emergency Medicine, Royal Blackburn Hospital, United Kingdom.
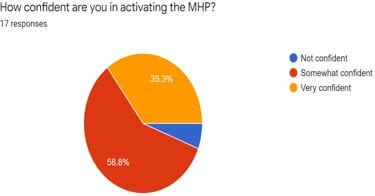
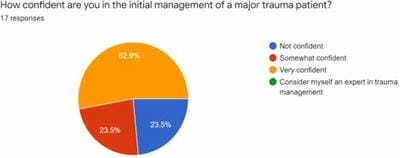
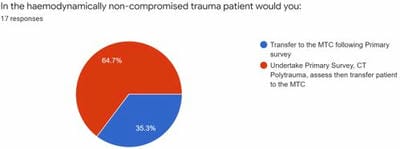
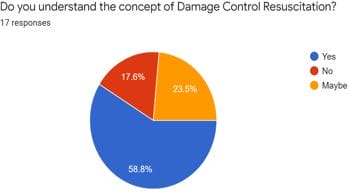
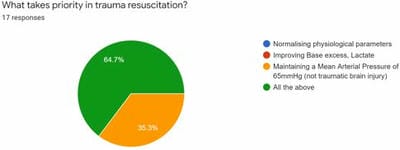
Introduction: We recognised there was a need for a set criterion for the activation of MHP and MTTA at our Trust. The main aim is to streamline the trauma care that our patients would receive around the clock. Ours is a large Major Trauma Unit regularly receiving a large volume of trauma patients of varying severity of injury Objective: The use of a checklist for the initial management of MTTA and MHP to ensure the process is streamlined and led by the trauma team leader. This would help reduce the cognitive load that is often presented to the team leader. This would also help direct junior team members with limited experience in the initial management of major trauma. Method/Intervention: An initial survey about MTTA and MHP from senior clinicians was carried out. Several teaching sessions were undertaken. In addition to this, an algorithm for the initial management in terms of transfer protocol was also introduced. Results: From the clinicians’ perspective, 89% of the respondents felt that the use of MHP and MTTA protocol would reduce the cognitive load whilst managing major trauma. There was an improvement in the level of confidence of clinicians in the initial management of major trauma from 52.9 % to 89%. Conclusion: Through this project, we hope that there is a better understanding of the need to have pre-defined criteria for activation for MTTA and MTP for several reasons as highlighted in the article. The eventual aim of the project is to streamline the initial management of the majorly injured patient and undertake the necessary practical steps.
Keywords: Major Trauma, Haemorrhage, Resuscitation
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Specialist Registrar, Emergency Medicine, Royal Blackburn Hospital, United Kingdom, , . Email:  |
Debkumar Chowdhury, Quality Improvement Project in the introduction of Major Trauma and Major Haemorrhage Protocol. Int J Med Res Rev. 2022;10(3):104-112. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1389 |
 |
 ©
©