A Rare Presentation of a Common Disease: A Diagnostic Dilemma
Maitra S.1*, Yusuf S.2, Ray K.3, Singla R.4, Krishna De J.5, Basu S.6
DOI: https://doi.org/10.17511/ijmrr.2021.i06.08
1* Somnath Maitra, Associate Professor, Department of General Medicine, JIMSH Budge, Kolkata, West Bengal, India.
2 Sk Adnan Yusuf, Senior Resident, Department of General Medicine, JIMSH Budge, Kolkata, West Bengal, India.
3 Koushik Ray, Assistant Professor, Department of Anatomy, JIMSH Budge, Kolkata, West Bengal, India.
4 Rahul Singla, Senior Resident, Department of Radiology, JIMSH Budge, Kolkata, West Bengal, India .
5 Jiban Krishna De, Professor, Department of Radiology, JIMSH Budge, Kolkata, West Bengal, India.
6 Subhadeep Basu, 2nd year DNB PGT, Department of General Medicine, JIMSH Budge, Kolkata, West Bengal, India.
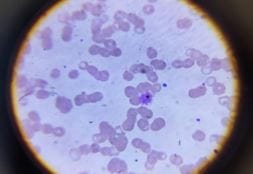
Malaria affects millions of people across the globe. The classical clinical features may be absent, but the rapid diagnosis helps in early treatment and thus avoids complications. We present a case of co-infection of Plasmodium vivax and Plasmodium falciparum malaria in a female patient presenting with fever and pain abdomen and incidental detection of the splenic infarct. The co-infection is uncommon and treatment should target both to avoid complications. Also, the exact pathogenesis is un known and though splenic infarct is uncommon and missed due to lack of symptoms, it should be followed up.
Keywords: Co-infection, Plasmodium vivax, Plasmodium falciparum, Splenic infarct
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of General Medicine, JIMSH Budge, Kolkata, West Bengal, India. Email:  |
Somnath Maitra, Sk Adnan Yusuf, Koushik Ray, Rahul Singla, Jiban Krishna De, Subhadeep Basu, A Rare Presentation of a Common Disease: A Diagnostic Dilemma. Int J Med Res Rev. 2021;9(6):399-402. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1358 |
 |
 ©
©