Clinico-Histopathological Correlation of Non-Neoplastic Dermatological Lesions
Kumar V.1, Sharan A.2, Poriya S.3, kundu S.4*
DOI: https://doi.org/10.17511/ijmrr.2022.i01.04
1 Vibhuti Kumar, Chief of lab, , Dr Lal Path Lab, Purnea, Bihar, India.
2 Anita Sharan, Professor, Department of Pathology, D.Y. Patil University School of Medicine, Nerul, Navi Mumbai, India.
3 Sunita Poriya, Assistant Professor, , Geetanjali Medical College, Udaipur, Rajasthan, India.
4* Sonia kundu, Additional Senior Medical Officer, , Civil Hospital, Panipat, Haryana, India.
Objective: Non-neoplastic skin disorders are more common than neoplastic skin disorders which have included Infectious diseases, non-infectious erythematous lesions, papular & squamous disorders, connective tissue diseases, non-infectious vesiculobullous / Vesiculopustular disorders e.tc. The pattern of skin diseases varies from one country to another and across different parts of the same country. So due to the variable spectrum, the histopathology of skin diseases is varied. Each clinical presentation is common to different histopathological pictures & thus definitely requires histopathology for confirmation. Design: This study was conducted by Dr D. Y. Patil Medical College and Hospital, Navi Mumbai from October 2018 to October 2020. Subjects: One hundred and fifty non-neoplastic specimens of skin biopsies submitted in the histopathology; Department of Pathology were considered as the subjects of the study. Material and Methods: Histopathological results were presented in tabular and graphical forms. Mean, median, standard deviation and ranges were calculated for quantitative data. The Chi-square test and t-test with p<0.001 was considered significant. Results: The mean age of our study participants was 41.9 years with a standard deviation of 36.5 years. The majority of our study participants were females: 29.4 % of patients presented with infectious lesions, 22.7 % of patients presented with papulosquamous lesions, and 12.7 % of patients presented with vesiculobullous lesions. The most common infectious non-neoplastic skin lesion was leprosy, the most common papulosquamous skin lesion was dermatitis, and the commonest vesiculobullous skin lesion was Pemphigus Vulgaris. Conclusion: An integrated approach by dermatologists and pathologists is recommended to increase the accuracy of diagnosis and for better management of the patient.
Keywords: Leprosy, Non-Neoplastic skin lesions, Psoriasis, Papulo-squamous lesions, Vesicobullous lesions
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Additional Senior Medical Officer, , Civil Hospital, Panipat, Haryana, India. Email:  |
Vibhuti Kumar, Anita Sharan, Sunita Poriya, Sonia kundu, Clinico-Histopathological Correlation of Non-Neoplastic Dermatological Lesions. Int J Med Res Rev. 2022;10(1):24-30. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1351 |
 |
 ©
© 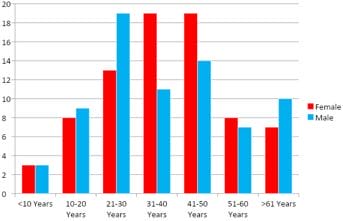 Figure 1: Bar graph showing age and sex distribution of skin lesions.
Figure 1: Bar graph showing age and sex distribution of skin lesions.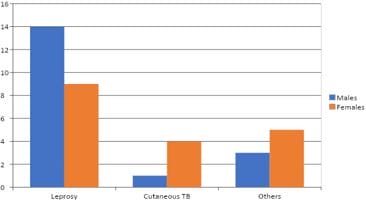 Figure 2: Graph showing distribution of infectious skin lesions with gender.
Figure 2: Graph showing distribution of infectious skin lesions with gender.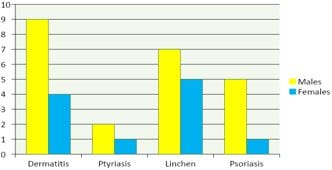 Figure 3: Bar graph showing the distribution of papulosquamous skin lesions with gender.
Figure 3: Bar graph showing the distribution of papulosquamous skin lesions with gender.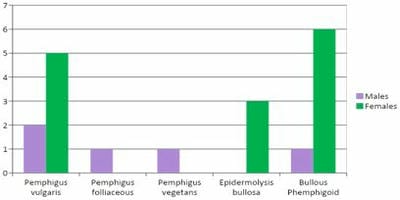 Figure 4: Bar graph showing the distribution of vesicobullous skin lesions with gender.
Figure 4: Bar graph showing the distribution of vesicobullous skin lesions with gender.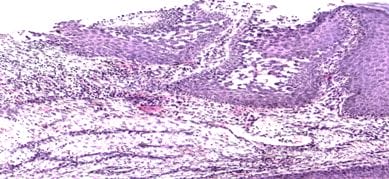 Figure 5: Pemphigus Vegetans: Suprabasal acantholysis with pseudo-epitheliomatous hyperplasia.H & E 100X.
Figure 5: Pemphigus Vegetans: Suprabasal acantholysis with pseudo-epitheliomatous hyperplasia.H & E 100X.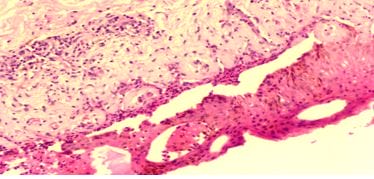 Figure 6: Bullous Pemphigoid: Lymphocytes and eosinophils are present at the dermo-epidermal junction.Eosinophilic spongiosis. H & E 100X.
Figure 6: Bullous Pemphigoid: Lymphocytes and eosinophils are present at the dermo-epidermal junction.Eosinophilic spongiosis. H & E 100X.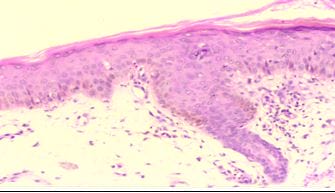 Figure 7: Guttate Psoriasis: Blunting of rete ridges, orthokeratosis, slight acanthosis, dilated blood vessels in dermal papillae. H & E 100X.
Figure 7: Guttate Psoriasis: Blunting of rete ridges, orthokeratosis, slight acanthosis, dilated blood vessels in dermal papillae. H & E 100X.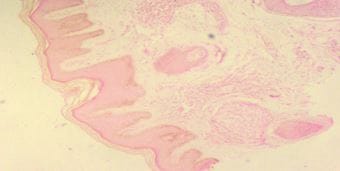 Figure 8: Indeterminate Leprosy: Orthokeratotic, hyperkeratosis, irregular acanthosis and mild spongiosis. Pandermal perineurovascular and periappendegeal chronic inflammation. H&E 40X.
Figure 8: Indeterminate Leprosy: Orthokeratotic, hyperkeratosis, irregular acanthosis and mild spongiosis. Pandermal perineurovascular and periappendegeal chronic inflammation. H&E 40X.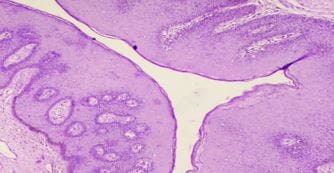 Figure 9: Condyloma Acuminata: Papillomatosis and acanthotic squamous epithelium. Vacuolated and round hyperchromatic nuclei. H&E 40X.
Figure 9: Condyloma Acuminata: Papillomatosis and acanthotic squamous epithelium. Vacuolated and round hyperchromatic nuclei. H&E 40X.