Risk Factors Affecting Exacerbation of Bronchiectasis Leading to Hospitalisation in Patients Attending a Tertiary Care Setting
Ettuveetil M.1, Anandan P.2*, Akkara P.3
DOI: https://doi.org/10.17511/ijmrr.2021.i06.05
1 Mahroofa Ettuveetil, Senior Resident, Department of Pulmonary medicine, Govt. Medical College, Manjeri, Malappuram, Kerala, India.
2* Poriyanganattu Thankappan Anandan, Associate Professor, Department of Pulmonary medicine, Govt. Medical College, Kozhikode, Kerala, India.
3 Paulo Varghese Akkara, Assistant Professor, Department of Pulmonary medicine, Govt. Medical College, Kozhikode, Kerala, India.
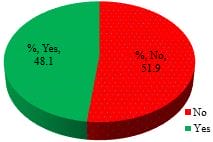
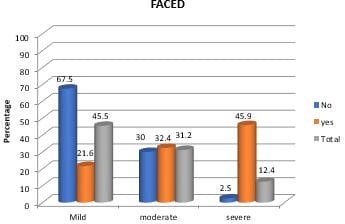
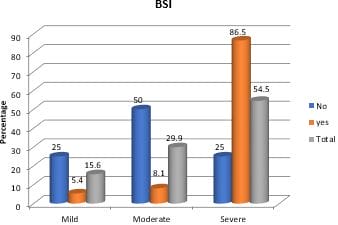
Introduction: Bronchiectasis is a chronic respiratory disease characterized by structural changes in airways, leading to recurrent episodes of cough with expectoration. Exacerbations are significant events associated with increased morbidity and mortality. Aim: To evaluate factors associated with exacerbations requiring hospitalization in patients with bronchiectasis Materials and methods: A prospective observational study was done at a tertiary care teaching hospital from December 2017 to May 2019. Demographic data, comorbidities, investigations including HRCT, sputum culture and spirometry were collected. Patients were grouped into exacerbations requiring hospitalizations and those managed as outpatients and followed up for one year. Factors associated with exacerbations were assessed and compared between the two groups. Results: 89 patients were recruited for the study, out of which 12 patients without exacerbation during the study period were excluded. The remaining 77 patients were divided into those who needed hospitalization (37) and those managed as outpatients (40). About 48.1%required hospital admission. Factors associated with exacerbations were advanced age, isolation of organisms from sputum, FEV1 less than 50%, PPI use during the study period, concomitant COPD, vaccination with pneumococcal and influenza vaccines and high severity scores. Use of LTO2, LABA/ICS, chest physiotherapy, mucolytic agents, radiological extent and previous history of exacerbations were not associated with exacerbations leading to hospitalization. Conclusion: Factors associated with bronchiectasis exacerbations leading to hospitalizations were advanced age, high bronchiectasis severity score, FEV1 less than 50%, PPI use and concomitant COPD. Vaccination for influenza and pneumococcus had a favourable impact in reducing hospitalization.
Keywords: Bronchiectasis, Exacerbation, Hospitalization
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Pulmonary medicine, Govt. Medical College, Kozhikode, Kerala, India. Email:  |
Mahroofa Ettuveetil, Poriyanganattu Thankappan Anandan, Paulo Varghese Akkara, Risk Factors Affecting Exacerbation of Bronchiectasis Leading to Hospitalisation in Patients Attending a Tertiary Care Setting. Int J Med Res Rev. 2021;9(6):379-387. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1349 |
 |
 ©
©