Clinicopathological analysis of 33 cases of laryngeal carcinoma with their response to COVID19 virus
Elmatri H.1*, Gheryani N.2
DOI: https://doi.org/10.17511/ijmrr.2021.i06.06
1* Houssein Elmatri, Associate professor, Department of Otolaryngology, Faculty of Medicine, University of Benghazi, Benghazi, Libya, North Africa. ORCID ID: 0000-0002-7775-1916
2 Nabeia Gheryani, Associate professor, Department of Pathology, Faculty of Medicine, University of Benghazi, Benghazi, Libya, North Africa. ORCID ID: 0000-0001-6535-6882
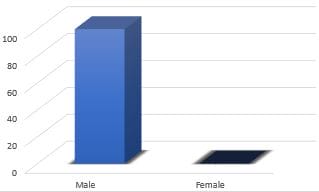
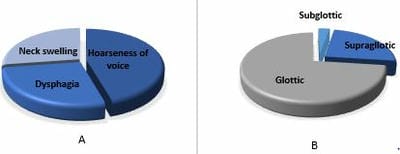
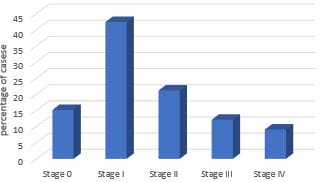
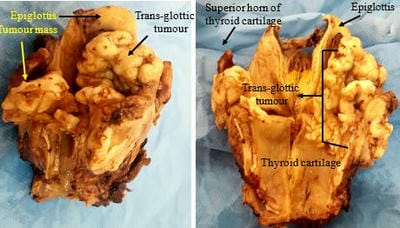
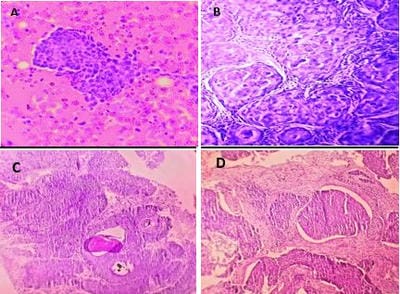
Background: laryngeal carcinoma is a common cancer of the head and neck region. Lifestyle, signs and symptoms, including those of COVID-19, clinical and histological features of the lesions were highlighted in this study to increase the understanding of this fatal cancer, which will decrease the high morbidity and mortality rates associated with it. Methods: This study was conducted at the Department of Otorhinolaryngology, 33 cases of laryngeal cancer presented from January 2017 to July 2019 were included in this study. Results: the leading age group of subjects was 51-60 years. Smoking was a significant risk factor in 100% of cases. Most of the patients presented with hoarseness of voice followed by dysphagia. The glottic area was the commonest site (72.7%) for laryngeal cancer and squamous cell carcinoma seen in 100% of patients. Most of the cases showed a well-differentiated tumour with 39.9% of patients and presented in stage I (42.4%). Only a few cases (9%) had cervical lymph node metastasis at the time of presentation. And only four patients developed COVID-19 infection post laryngectomy, their symptoms were mild upper respiratory tract infection, and their chest x-rays were clear. All of them healed without any severe complication of CVOID-19. Conclusions: Early detection of laryngeal cancer is associated with a good prognosis. This early detection is based on good history, clinical examination, and invasive and non-invasive investigation. Post laryngectomy care may play an essential role in protecting the patient from serious complications of COVID-19 infection.
Keywords: COVID-19, Laryngeal carcinoma, Smoking
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate professor, Department of Otolaryngology, Faculty of Medicine, University of Benghazi, Benghazi, Libya, North Africa. Email:  |
Houssein Elmatri, Nabeia Gheryani, Clinicopathological analysis of 33 cases of laryngeal carcinoma with their response to COVID19 virus. Int J Med Res Rev. 2021;9(6):388-394. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1348 |
 |
 ©
©