A study to assess the practice of biomedical waste management and its influencing factors among health care providers at selected hospitals of Kolkata, West Bengal
Moyon N.1, Devi K.2*
DOI: https://doi.org/10.17511/ijmrr.2021.i06.02
1 Ngamning Ngoruw Moyon, MSc Nurse, Medical-Surgical Speciality, , , , .
2* Khumukcham Anupama Devi, Tutor, Child Health Nursing Department, College of Nursing, A.I.I.M.S, Patna, Bihar, India.
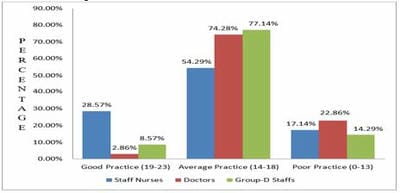
Background: Mismanagement of healthcare waste puts the community, the patients and healthcare workers at risk, both in terms of the risks from inadequate storage, transportation and disposal of infectious waste and from the environmental risks arising from hazardous burning. A descriptive survey was undertaken to assess the practice of Biomedical Waste Management and its influencing factors among health care providers. Method: Quantitative, non-experimental Survey Research Design was adopted. A total of 105 health care providers, namely the Staff Nurses, Doctors and Group-D staff, were selected by convenient sampling technique from three government hospitals. Descriptive and inferential statistics were used for data analysis. Result: The study findings revealed that the mean practice scores for Staff Nurses, Doctors and Group-D staff were 16.66, 14.77 and 16.03, respectively. There was a statistically significant association between the practice score of Staff Nurses and their age (χ2(1) = 8.11, p<0.05) and period of working experience in the hospital setup (χ2(1) = 8.24, p<0.05). The factors like unawareness (28.6%), lack of training or in-service education (41.9%), overload of work (61%), lack of supervision (36.2%), lack of audit (36.2%), lack of supplies (61.9%) as expressed by the health care providers also emerged from the study which is probably the negative factors leading to their average practice and poor practice. Conclusion: From the study findings, it can be concluded that only a few of the practices of health care providers were good, of which Staff Nurses were the majority group who adhere to good practices.
Keywords: Biomedical Waste Management, Factors influencing, Health Care Providers, Practice
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Tutor, Child Health Nursing Department, College of Nursing, A.I.I.M.S, Patna, Bihar, India. Email:  |
Ngamning Ngoruw Moyon, Khumukcham Anupama Devi, A study to assess the practice of biomedical waste management and its influencing factors among health care providers at selected hospitals of Kolkata, West Bengal. Int J Med Res Rev. 2021;9(6):357-367. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1332 |
 |
 ©
©