Management of multiple rib fractures-results from a Major Trauma Centre with the review of the existing literature
Chowdhury D.1*, Okoh P.2, Dambappa H.3
DOI: https://doi.org/10.17511/ijmrr.2020.i06.01
1* D. Chowdhury, Specialty Registrar, Emergency Medicine, Royal Preston Hospital, England, United Kingdom.
2 P. Okoh, Specialty Registrars, Emergency Medicine, Royal Preston Hospital, England, United Kingdom.
3 H. Dambappa, Specialty Registrars, Emergency Medicine, Royal Preston Hospital, England, United Kingdom.
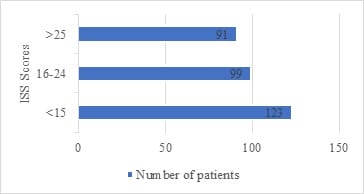
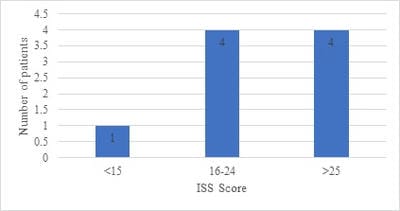
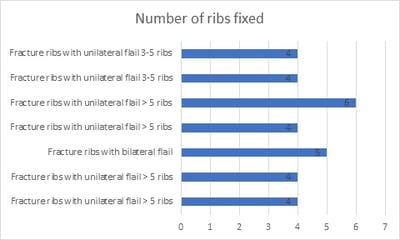
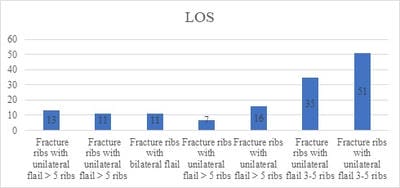
Introduction: Rib fractures are amongst the most common fractures following major trauma presenting to the Emergency Department. The impact of rib fractures is even more significant in the patient with underlying chronic respiratory conditions. Aim: To assess our current management of rib fractures at our trauma center. Method: The current study collected our data from the TARN Registry primarily focussing on patients with multiple rib fractures. The main components were the analgesic requirement of our patients. The number of rib fracture stabilization procedures and the average number of ribs fixed were also studied. Results: The data were collected retrospectively over 12 months. There were 313 patients identified as having chest wall injuries. From the data, 41.9% (131) of patients were over the age of 65 years. A significant proportion of our patients 34.5% (108) were noted to have multiple rib fractures (>3 Ribs). It was noted that 3% (9) of the 313 patients required operations. The average of the patients included in the study was noted to be 61 years with an age range of 17-92 years. Conclusion: The mainstay management of rib fracture is a provision of adequate analgesia and the prevention of respiratory complications that can all stem from poor ventilatory function amongst other patient factors and injury patterns. Through the decades, surgical stabilization has gained pace and has found its niche in the management of rib fractures.
Keywords: Rib Fracture, Trauma, Pain Management
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Specialty Registrar, Emergency Medicine, Royal Preston Hospital, England, United Kingdom. Email:  |
Chowdhury D, Okoh P, Dambappa H. Management of multiple rib fractures-results from a Major Trauma Centre with the review of the existing literature. Int J Med Res Rev. 2020;8(6):379-385. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1227 |
 |
 ©
©