Serum calcium and magnesium levels in acute gastroenteritis
Kumar Patel N.1, Kumar Kedia M.2, Majhi C.3, Kumar Bariha P.4, Oram G.5*
DOI: https://doi.org/10.17511/ijmrr.2020.i06.07
1 Nayan Kumar Patel, Assistant Professor, Department of Cardiology, Veer Surendra Sai Institute Of Medical Sciences And Research, Burla, Odisha, India.
2 Madhav Kumar Kedia, Senior Resident, 3 Chakradhar Majhi, Associate Professor, 4 Prafulla Kumar Bariha, Assistant Professor, 5* Gouri Oram, Assistant Professor; all authors are affiliated with Department of General Medicine, Veer Surendra Sai Institute Of Medical Sciences And Research, Burla, Odisha, India.
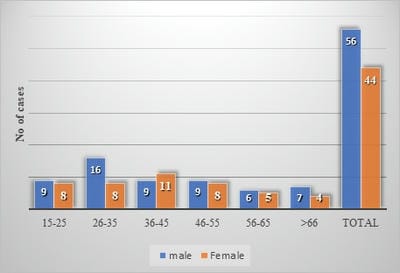
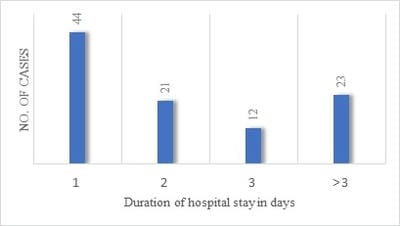
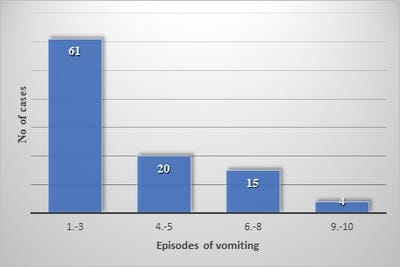
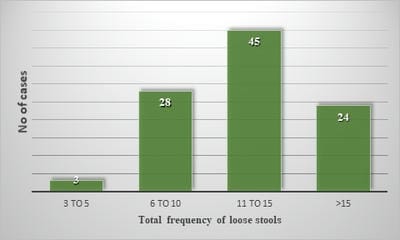
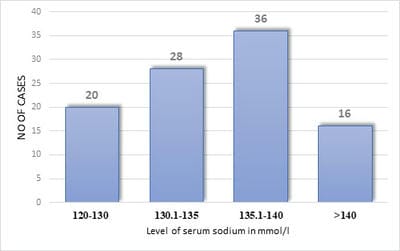
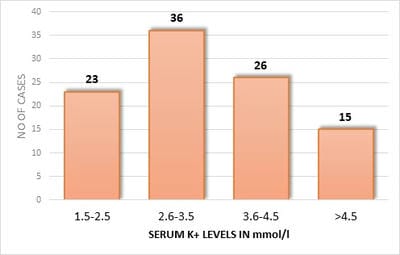
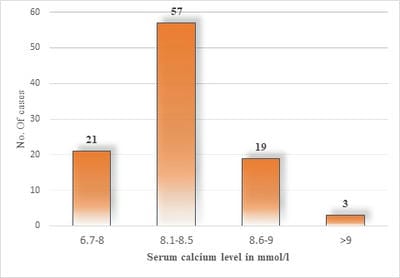
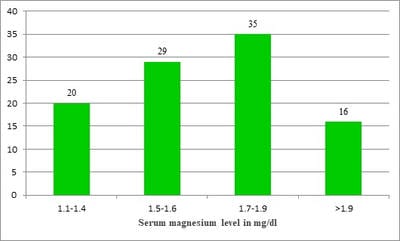
Background: Acute diarrhea endemic in India has a prevalence of 7% which is commonly seen in children and also is a major problem in adults. Acute diarrhea with dehydration culminates in the loss of electrolytes. Not only Na+ K+ but also Ca2+and Mg2+ are also substantially lost and lead to symptoms and adds to morbidity and prolong hospitalization. Methods: In this observational study, a total of 100 cases of acute gastroenteritis admitted to the department of general medicine and infectious disease ward of VIMSAR, Burla, between November 2018 to December 2019 were investigated clinically and biochemically and data were interpreted statistically. Results: Males (56%) were more in number than females (44%), were mostly in the age group of 26-35 years (24%). Hypocalcemia, hypokalemia, hypomagnesemia, and hyponatremia were found in 97%, 59%, 49%, 48% of cases respectively. Correlation of Serum Ca2+with (r-value) total episodes of vomiting (-0.536), total episode of stools (-0.880), S. Na+ level (-0.374), S. K+ level (-0.729), with the duration of hospital stay (-0.770) respectively. Correlation of S. Mg2+ levels with (r-value) total episodes of vomiting (-0.475), total episode of stools (-0.498), S. Na+ level (-0.301), S. K+ level (-0.801), duration of hospital stay (-0.699) respectively. The correlations were found to be statistically highly significant (with a p-value is <0.01). Conclusion: Early detection and prompt correction of electrolytes will be beneficial, as it will decrease the duration of hospital stay, morbidity, mortality, thereby, decrease the burden on the health system of the country.
Keywords: Acute Gastroenteritis, Correlation, S. Calcium, S. Magnesium
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of General Medicine, Veer Surendra Sai Institute Of Medical Sciences And Research, Burla, Odisha, India. Email:  |
Patel NK, Kedia MK, Majhi C, Bariha PK, Oram G. Serum calcium and magnesium levels in acute gastroenteritis. Int J Med Res Rev. 2020;8(6):416-423. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1224 |
 |
 ©
©