Estimation of prostate size by trans-rectal ultrasound and its correlation with DRE and endoscopic grading
Gupta S.1, Saraf S.2, Kumar Pal D.3*
DOI: https://doi.org/10.17511/ijmrr.2020.i01.10
1 Sandeep Gupta, Associate Professor, Department of Urology, Institute of Post Graduate Medical Education & Research, Kolkata, West Bengal, India.
2 Siddharth Saraf, Post-Doctoral Trainee, Department of Urology, Institute of Post Graduate Medical Education & Research, Kolkata, West Bengal, India.
3* Dilip Kumar Pal, Professor & Head, Department of Urology, Institute of Post Graduate Medical Education & Research, Kolkata, West Bengal, India.
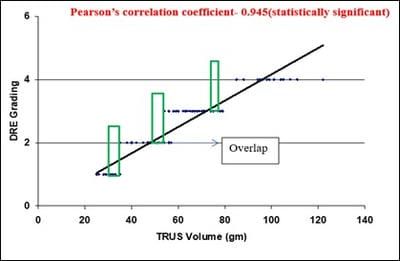
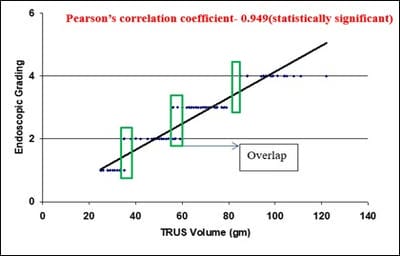
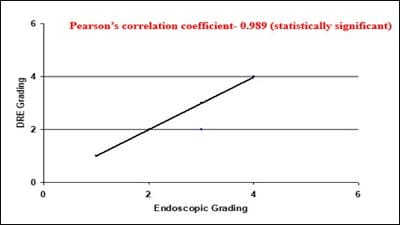
Aim: Digital rectal examination (DRE) grading and the grade of prostatomegaly on cystoscopy are routinely used in clinical practice, but its correlation to prostate volume is understudied. This study was done to assess the correlation of DRE and endoscopic grading with the prostate volume on trans-rectal ultrasound (TRUS). Materials and Methods: This study was carried out in 101 eligible patients with prostatomegaly. Each patient was evaluated for three parameters, prostate volume by TRUS examination, DRE and endoscopic grading on cystoscopy. Pearson correlation coefficient was calculated to find the correlation between variables, p<0.05 was taken to be statistically significant. Data were analyzed using the Epi Info (TM) 7.2.2.2. Results: Significant positive correlation (p<0.001) was found between TRUS Volume and DRE grading (Pearson Correlation=0.945) and TRUS volume and Endoscopic grading (Pearson Correlation=0.949). Both the grading were also significantly positively correlated (Pearson Correlation=0.989, p<0.001). Conclusion: Our attempt for correlating the digital rectal grading and endoscopic grading with prostate volume is satisfactorily validated in the clinical setting. These grades are sufficient to provide a rough estimation of the prostate volume and to classify patients with prostatomegaly.
Keywords: DRE, TRUS, Endoscopic grading, Prostate size
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor & Head, Department of Urology, Institute of Post Graduate Medical Education & Research, Kolkata, West Bengal, India. Email:  |
Gupta S, Saraf S, Pal DK. Estimation of prostate size by trans-rectal ultrasound and its correlation with DRE and endoscopic grading. Int J Med Res Rev. 2020;8(1):63-68. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1140 |
 |
 ©
©