Study of fine needle aspiration cytology evaluation of peripheral lymph nodes
Gayen P.1, Ghosh S.2*, Naskar S.3
DOI: https://doi.org/10.17511/ijmrr.2019.i04.02
1 Prosenjit Gayen, Assistant Professor, Department of Pathology, Malda Medical College, Malda, West Bengal, India.
2* Saswata Ghosh, Assistant Professor, Department of Chest Medicine, Malda Medical College, Malda, West Bengal, India.
3 Subhrajyoti Naskar, Assistant Professor, Department of Community Medicine, Malda Medical College, Malda, West Bengal, India.
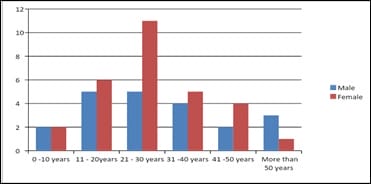
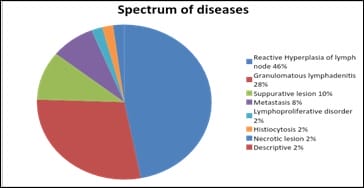
Introduction: Lymph nodes are an integral component of the immune system and their enlargement is commonly noted in clinical practice in a wide spectrum of diseases, including infections like tuberculosis and malignancy. FNAC is an important diagnostic tool for rapid evaluation of mainly superficial lesions, especially of lymph nodes. It is cost effective, relatively less traumatic, and enables the pathologist to provide the clinician with a diagnosis in a very short time, and hence is ideal especially for OPD patients. Objectives: 1. To study the age and sex distribution of the patients of FNAC of peripheral lymph node. 2. To study the spectrum of diseases diagnosed on FNAC of peripheral lymph nodes. Methods: Cross-sectional hospital based Observational study. Total 50 patients who had superficial lymphadenopathy were included in this study. Male patients were 21 (42%) and Female patients were 29 (58%). FNAC was performed on this 50 patients. Diagnosis was made by light Microscopy. Result was tabulated and statistical analysis was done. Results: Male patients were 21 (42%) and Female patients were 29 (58%). 50 % patients were in the age group of 21 to 40 years. Reactive hyperplasia was 46% and Granulomatous lymphadenitis was 18%. Cervical lymph nodes were most commonly involved. Conclusion: FNAC is a simple, quick, low cost, minimally invasive and easy diagnostic procedure which is very much helpful in the diagnosis of diseases causing superficial lymphadenopathy in all age groups. Reactive hyperplasia of lymph node was the most common cytological diagnosis followed by Granulomatous lymphadenitis.
Keywords: FNAC, Granulomatous lymphadenitis, Lymph node, Reactive hyperplasia
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Chest Medicine, Malda Medical College, Malda, West Bengal, India. Email:  |
Gayen P, Ghosh S, Naskar S. Study of fine needle aspiration cytology evaluation of peripheral lymph nodes. Biomed Rev J Basic Appl Med Sci. 2019;7(4):259-265. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1067 |
 |
 ©
©