Individualised Homoeopathic Medicines Alleviated the Recurrent Epistaxis in Identical Twins with Severe von Willebrand Disease and Haemophilia A: A Duo Case Report
Tapas K1, Kumat O2*, Kalda P3, Aswar C4
DOI:https://doi.org/10.17511/ijmrr.2025.i01.03
1 Kundu Tapas, Principal Investigator and Prof and HOD, Homoeopathy In Haemophilia and Physiology Department, Motiwala Homoeopathic Medical College, Nashik, Maharashtra, India.
2* Omkar Kumat, Communication Consultant and Assistant Professor, Physiology Department, Smt KB Abad Homoeopathy Medical College and Hospital Chandwad, Nashik, Maharashtra, India.
3 Prapti Kalda, Research Associate, Homoeopathy In Haemophilia.
4 Chandrakant Aswar, Principaland Prof and HOD, Physiology and Biochemistry, Takhatmal Shrivallabh Homoeopathic College and Hospital Rajapeth, Amravati, Maharashtra, India.
Background: von Willebrand Disease (vWD) is an inherited genetic bleeding disorder that prevents the blood from clotting. The prevalence of vWD is estimated to be approximately 1% of the population (or 10,000 cases per million population). The vWF binds and stabilizes blood clotting factor (FVIII) in circulation and therefore it helps in clot formation.
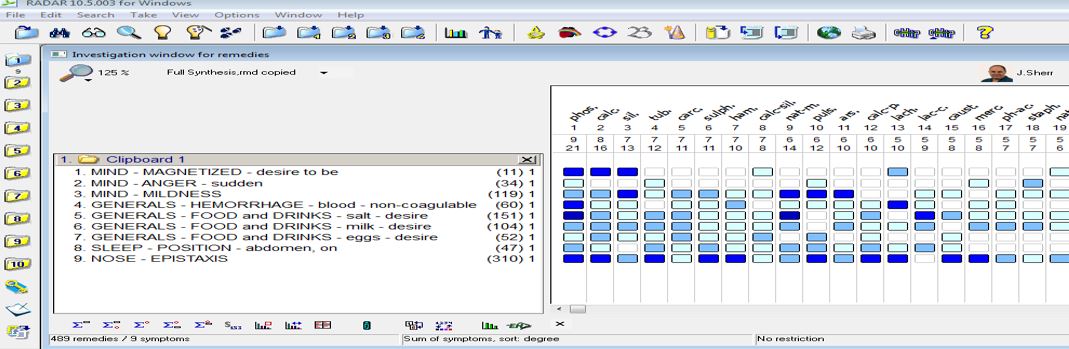
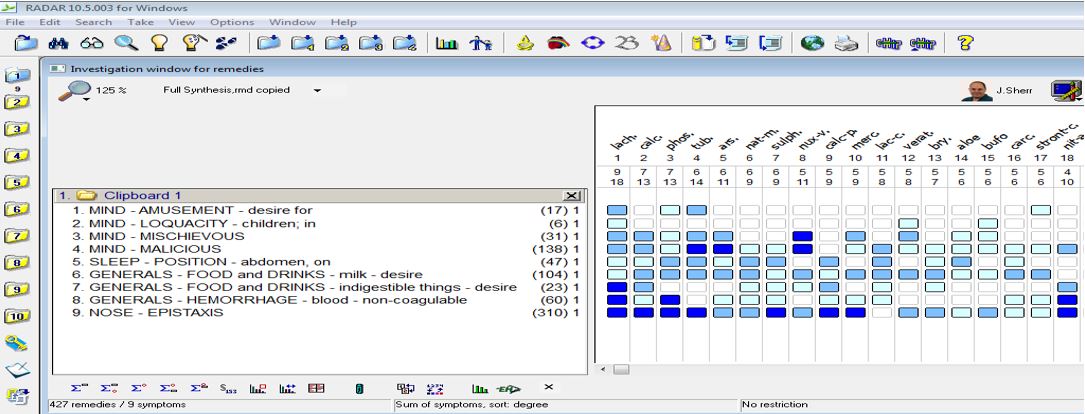
Case Profiles: This duo case report is the classical example of the association of vWD with haemophilia A in identical twins, where both the patients shared the same disease pattern and manifestations like recurrent epistaxis & ecchymotic patches. But when it came to homoeopathic prescription both of them were prescribed 2 different constitutional medicines based on their behaviour, constitution, etc.
Result and Discussion: The ISTH-BAT (International Society on Thrombosis and Haemostasis-Bleeding Assessment Tool) scale was used to measure the frequency of epistaxis and bruises which reduced from 6 to 1 in the elder twin and from 7 to 4 in the younger one. Modified Naranjo Criteria in Homoeopathy was used to assess the homoeopathic result with a score of 10 for the elder twin and 8 for the younger twin. This Duo Case Report signifies the role of two different Individualized Homoeopathic Medicines in identical twins though sharing a similar disease pattern.
Conclusion: Homoeopathic medicines prescribed based on individualization alleviated the genetic disease symptoms and improved the quality of life of the patients and the family members.
Keywords: von Willebrand Disease, Haemophilia A, Identical Twins, Individualized Homoeopathic Medicine
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Communication Consultant and Assistant Professor, Physiology Department, Smt KB Abad Homoeopathy Medical College and Hospital Chandwad, Nashik, Maharashtra, India. Email:  |
Tapas K, Kumat O, Kalda P, Aswar C, Individualised Homoeopathic Medicines Alleviated the Recurrent Epistaxis in Identical Twins with Severe von Willebrand Disease and Haemophilia A: A Duo Case Report. Int J Med Res Rev. 2025;13(1):11-18. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1532 |
 |
 ©
©