Correlation Between Airway Resistance as determined by R20 and Severity of Obstructive Sleep Apnea as Determined by Apnea-Hypopnea Index in Patients with Obstructive Sleep Apnea
Sasidharan A1*, Fathahudeen A2
DOI:https://doi.org/10.17511/ijmrr.2025.i01.08
1* Aswathy Sasidharan, Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
2 Fathahudeen A, Professor and Head of the Department, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
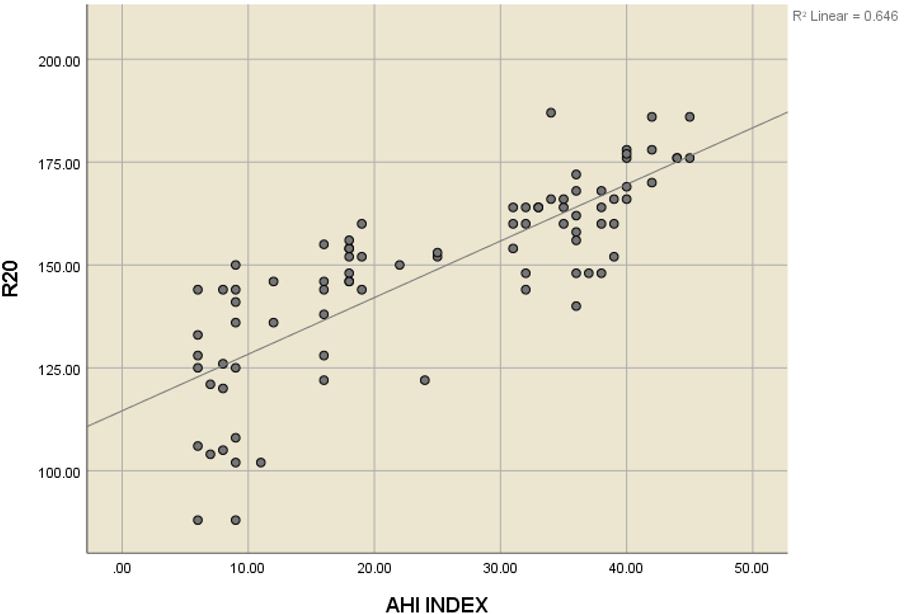
Background: Polysomnography is the gold standard for the diagnosis of patients with obstructive sleep apnea, but its routine use is limited by its cost. R20 measures the resistance of large central airways while R5 corresponds to total airway resistance, in large airway obstruction (as in OSA) central airway resistance (R20) increases and total resistance (R5) increases. This study aims to assess the usefulness of impulse oscillometry in the diagnosis of patients with obstructive sleep apnea, as it is a cost-effective, easy-to-perform investigation.
Materials And Methods: The present cross-sectional study included 85 patients suspected to have obstructive sleep apnea. Initial screening was done using the STOP BANG score. Specifically, patients with a score of 0 - 2 are considered at low risk for moderate to severe OSA, while those with a score of 5 -8 are classified as high risk for moderate to severe OSA and in our study those with a score ≥3 was advised to perform sleep study with their AHI index noted and subsequently impulse oscillometry noting their R20, R5 and R5-R20.
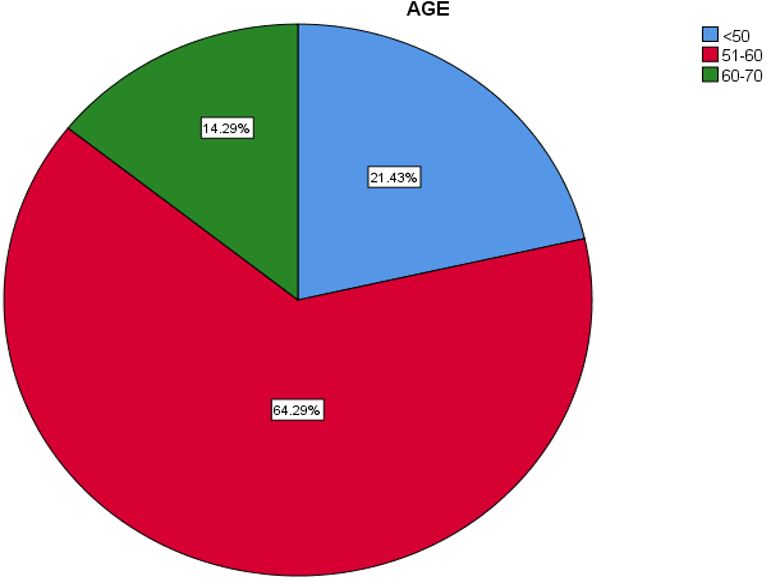
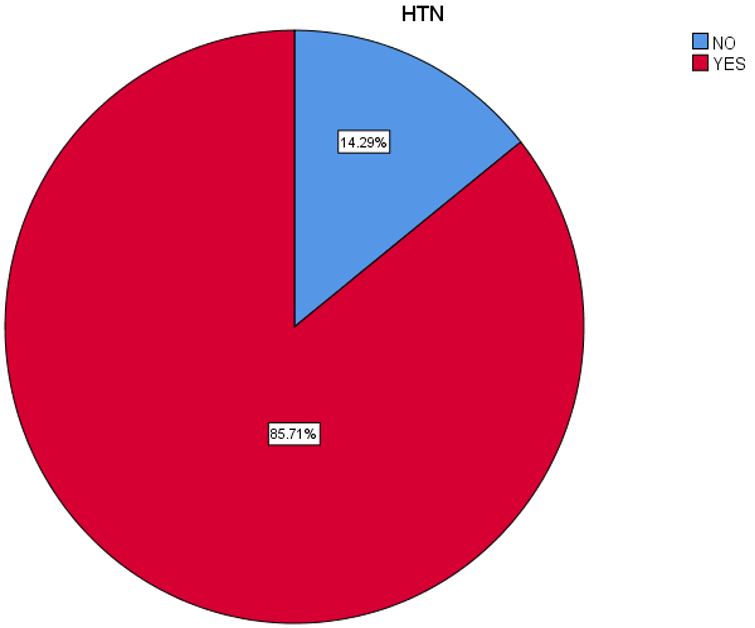
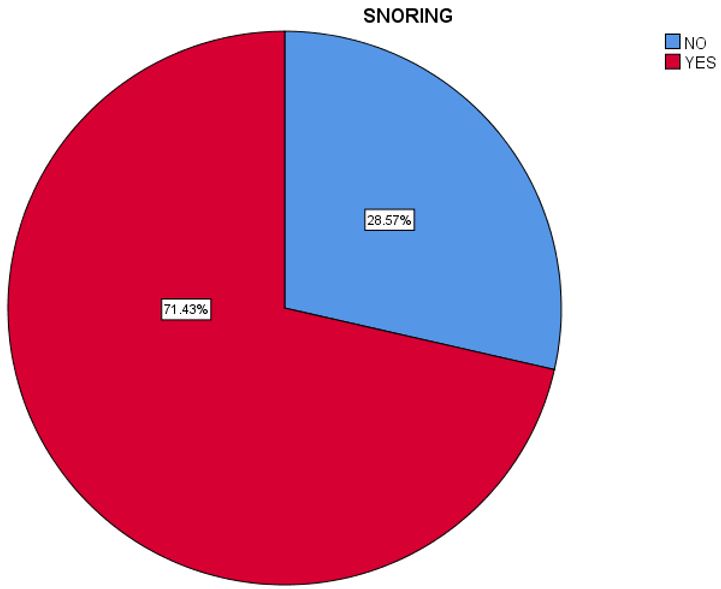
Results: In our study majority of participants (64.3%) fell within the 51-60 age range, which aligns with typical findings indicating a higher prevalence in middle-aged adults. The majority of participants,70 individuals were obese. In our study hypertension was the most prevalent comorbidity associated with OSA Among the 84 study subjects 63.1% of the sample, reported having Type 2 Diabetes Mellitus. 60 participants, making up 71.4% of the sample, reported that they do snore and we demonstrated a good correlation between the severity of OSA and snoring.
Conclusion: Impulse oscillometry can be a useful,easy-to-perform test in the evaluation of patients with OSA though further studies are needed.
Keywords: Obstructive sleep apnea , impulse oscillometry , ahi index
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India. Email:  |
Sasidharan A, Fathahudeen A, Correlation Between Airway Resistance as determined by R20 and Severity of Obstructive Sleep Apnea as Determined by Apnea-Hypopnea Index in Patients with Obstructive Sleep Apnea. Int J Med Res Rev. 2025;13(1):49-55. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1528 |
 |
 ©
©