Proportion Of Obstructive Airway Disease Among Post Pulmonary Tuberculosis Subjects in a Tertiary Care Setting
Akshaya KT1*, Fathahudeen A2, Kamala R3
DOI:https://doi.org/10.17511/ijmrr.2025.i01.07
1* Akshaya KT, Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
2 Fathahudeen A, Professor and Head of the Department, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
3 Kamala R, Assistant professor, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
Background: Pulmonary tuberculosis can affect lung function and the pulmonary function test of post-patients shows airway obstruction which is not reversible. This group of patients is in the category of post-TB obstruction syndrome with symptoms and signs similar to Chronic Obstructive Pulmonary Disease (COPD). The objectives of our study are: To determine the factors causing the development of obstructive airway disease in post-tuberculous individuals & To assess the severity of obstruction based on GOLD criteria.
Materials and Methods: The study was conducted in the Department of Pulmonary Medicine, Government Medical College Hospital, Thiruvananthapuram. This was a cross-sectional study that included patients with a history of pulmonary tuberculosis, (≥ 6 months after treatment), the pulmonary function test of each patient was assessed using spirometry as obstruction, restriction, mixed pattern or normal and in obstruction, the severity of obstruction was assessed as mild, moderate, severe, very severe based on GOLD criteria.
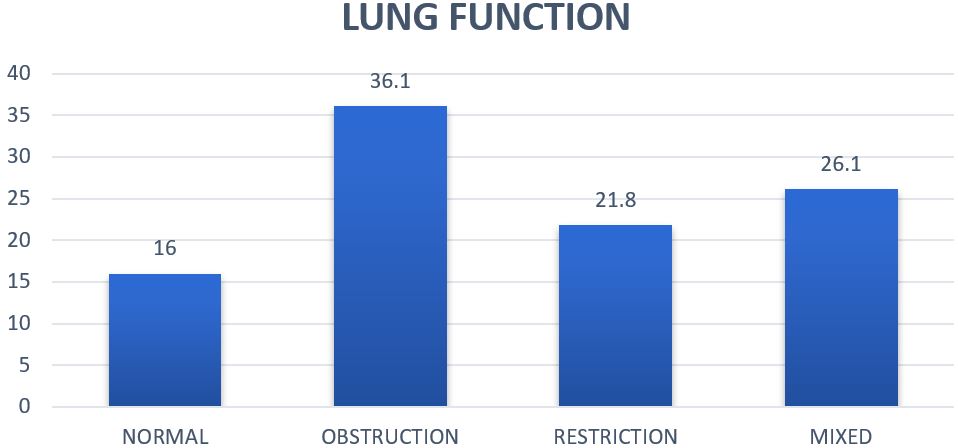
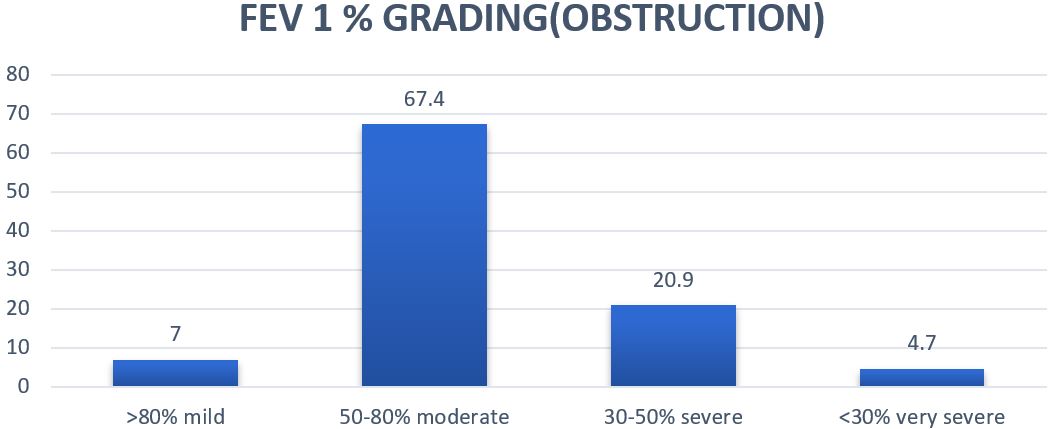
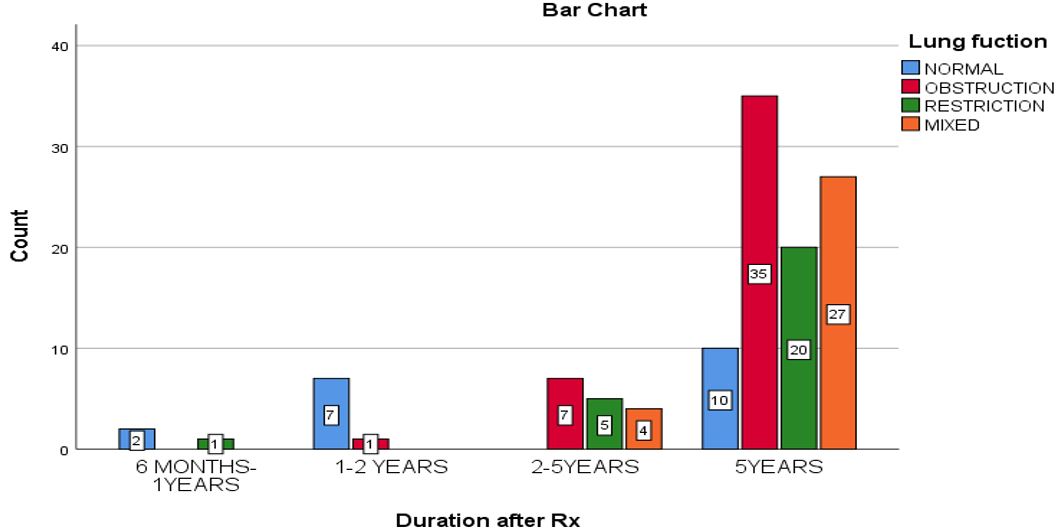
Results: In our study, 84% of patients had abnormal lung function, with obstruction as the predominant abnormality in 36%, 21.8% demonstrated restrictive abnormalities, and 26.1% showed mixed patterns. Among individuals with obstructive lung disease, the severity of obstruction was assessed based on their post-bronchodilator FEV1% according to GOLD grades for COPD. It was observed that 67.4% had moderate obstruction. The mean FEV1 for the moderate obstruction group, the most prevalent among obstructive cases, was 1.41 litres.
Conclusion: Patients with a history of pulmonary tuberculosis in the past, often present with signs of permanent impairment in lung function, which may manifest as obstruction, restriction, or a mixed pattern. Tuberculosis is an independent risk factor for the development of obstructive airway diseases.
Keywords: post tuberculosis, lung function, obstruction, airway diseases
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India. Email:  |
Akshaya KT, Fathahudeen A, Kamala R, Proportion Of Obstructive Airway Disease Among Post Pulmonary Tuberculosis Subjects in a Tertiary Care Setting. Int J Med Res Rev. 2025;13(1):42-48. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1520 |
 |
 ©
©