Hand Grip Strength As A Marker of Functional Impairment In Chronic Obstructive Pulmonary Disease Patients
Neena RS1*, Fathahudeen A2, Kamala R3
DOI:https://doi.org/10.17511/ijmrr.2025.i01.06
1* Neena RS, Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
2 Fathahudeen A, Professor and Head of the Department, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
3 Kamala R, Assistant professor, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India.
Background: COPD is a heterogeneous lung disease with multisystem involvement. COPD patients not only suffer from respiratory function impairment but also from peripheral muscle dysfunction which is an important manifestation that hinders day-to-day activities. Patients with a reduction in muscle strength should be detected early so that an early intervention through pulmonary rehabilitation can be done. pMDIs which is a common inhalation device in COPD require adequate hand strength for its actuation making the upper limb muscle strength an important parameter which is often ignored in COPD patients.
Objectives: To determine the hand grip strength of COPD patients objectively. To determine the association between hand grip strength with FEV1,6-minute walk distance and BODE index.
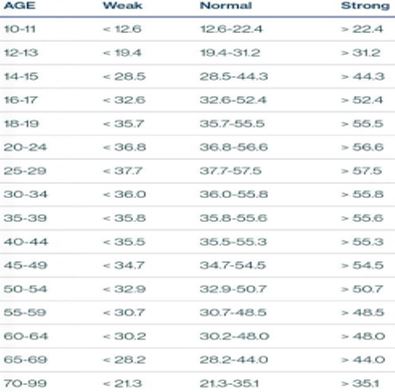
Methods: This is a cross-sectional followed by a prospective observational study conducted in the Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala. In 72 COPD patients, hand grip strength was assessed using a Camry Digital Dynamometer and was compared with the age and gender-adjusted values. Spirometry was done in all 72 patients and FEV1 measurement was recorded. A 6-minute walk distance was determined; the BODE index was calculated in these patients which comprises BMI, FEV1, Dyspnea on the MMRC scale and distance walked in 6 minutes.
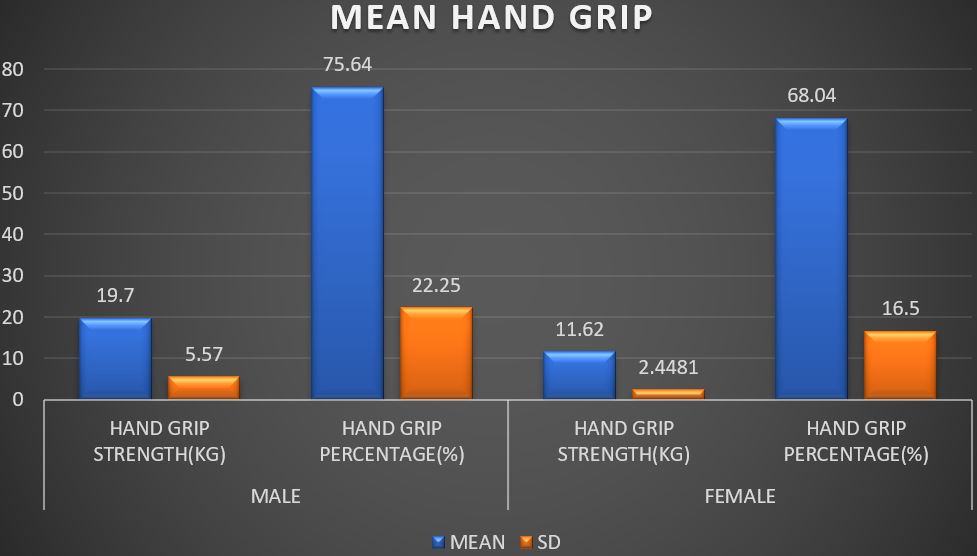
Results: COPD patients were found to have a reduction in their hand grip strength compared to their age and gender-adjusted values. In COPD patients, hand grip strength was found to have a positive correlation with a 6-minute walk distance whereas grip strength was found to have a negative correlation with BODE INDEX.
Conclusion: Hand grip strength is impaired in COPD patients and it could be used as a marker of functional impairment.
Keywords: Hand Grip Strength, COPD, FEV1, BODE Index
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate Resident, Department of Respiratory Medicine, Government Medical College, Trivandrum, Kerala, India. Email:  |
Neena RS, Fathahudeen A, Kamala R, Hand Grip Strength As A Marker of Functional Impairment In Chronic Obstructive Pulmonary Disease Patients. Int J Med Res Rev. 2025;13(1):33-41. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1519 |
 |
 ©
© 
 is 1.96 at 5% significance level; σ is 21.8 kg
is 1.96 at 5% significance level; σ is 21.8 kg