Clinical & Histopathological Profile Of Patients With Exudative Pleural Effusion Of Unknown Cause Who Undergo Medical Thoracoscopy
Kumar JVS1*, Fathahudeen A2
DOI:DOI:https://doi.org/10.17511/ijmrr.2025.i01.04
1* Jasti Venkata Suneel Kumar, Postgraduate Student, Department of Pulmonary Medicine, Government Medical College, Thiruvananthapuram, Kerala, India.
2 A Fathahudeen, Professor and Head of the Department, Pulmonary Medicine, Government Medical College, Thiruvananthapuram, Kerala, India.
Background: Exudative lymphocytic effusions form a significant proportion of undiagnosed pleural pathologies. This study explores the clinical and histopathological profile of exudative pleural effusion of unknown cause who undergo medical thoracoscopy.
Materials And Methods: This cross-sectional study enrolled 37 patients with exudative pleural effusion. Ultrasound-guided thoracentesis was conducted and samples were sent for pleural fluid cytology. Thoracoscopic pleural biopsy was kept as the gold standard.
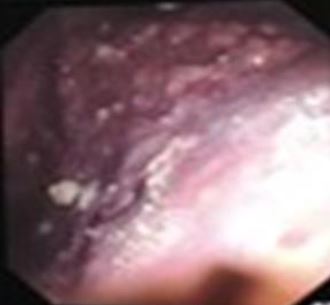
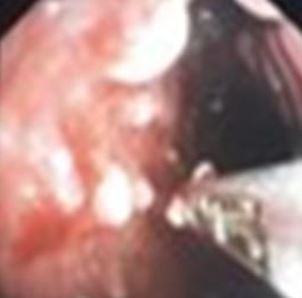
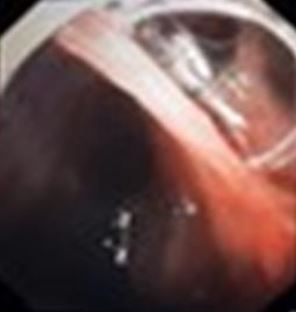
Results: A total of 37 patients were included in the study. 14 (37.83%) were smokers. 19 (51.35%) were exposed to firewood smoke. Only 1 participant (2.7%) reported exposure to passive smoke.5 patients had STEMI/ recent CABG in the last 1 year.1 participant reported a history of Ayurvedic drug intake. There was no asbestos occupational exposure in any of our subjects but 5 of our subjects had mesothelioma. It can be related to an indirect exposure which is absent due to a recall bias. 2 participants reported a history of recent trauma or RTA, but it was unrelated to the final diagnosis. Histopathological profile showed adenocarcinoma in 19(51.35%), tuberculosis in 7(18.9%).Thoracoscopy pleural findings include nodules in 26(70.27%).
Conclusion: Our study concluded that pleural nodules on thoracoscopy were suggestive of malignant aetiology with good cytology yield. Pleural metastasis from lung adenocarcinoma has a good yield of cytology and is the most common cause of exudative pleural effusions that underwent medical thoracoscopy.
Keywords: Medical thoracoscopy, HPE, Pleural Effusion
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate Student, Department of Pulmonary Medicine, Government Medical College, Thiruvananthapuram, Kerala, India. Email:  |
Kumar JVS, Fathahudeen A, Clinical & Histopathological Profile Of Patients With Exudative Pleural Effusion Of Unknown Cause Who Undergo Medical Thoracoscopy. Int J Med Res Rev. 2025;13(1):19-25. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1517 |
 |
 ©
©