The Outcome of Different Endoscopic Modalities in the Management of Large Proximal Ureteric Stone
Ali SMY1*, Islam MS2, Islam MS3, Jahan S4, Islam MR5, Miraj AKA6
DOI:https://doi.org/10.17511/ijmrr.2024.i06.03
1* S M Yunus Ali, Assistant Professor, Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
2 Md Saiful Islam, Professor, Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
3 Md Saiful Islam, Assistant Professor, Department of General Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
4 Salma Jahan, Associate Professor, Department of Nephrology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
5 Mohammed Rafiqul Islam, Assistant Professor, Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
6 A K Al Miraj, Research Assistant, Department of Vascular Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
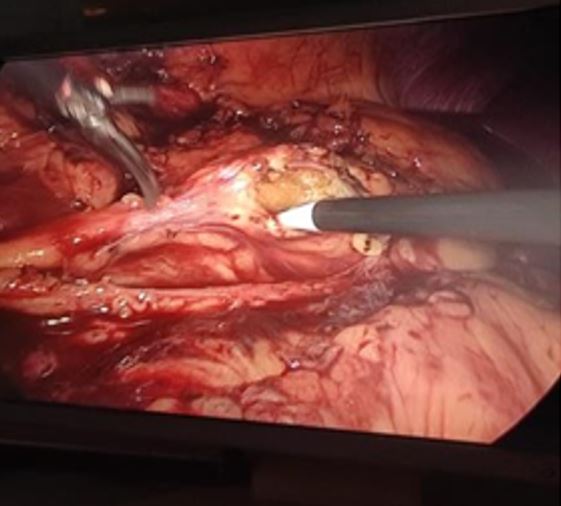
Background: Percutaneous nephrolithotomy. Various techniques have been documented for the management of Large Proximal Ureteric Stones (LPUS), such as laparoscopy (LUL), antegrade approach, retrograde ureteroscopy (RURS), extracorporeal shockwave lithotripsy, and infrequently open surgery. The paper compared the overall results of treating patients with large proximal ureteric stones (15-20 mm) using transperitoneal LUL, RURS, and mini-percutaneous antegrade ureteroscopy.
Methods: This prospective, randomised trial involved 100 individuals of both sexes who were above the age of 18 and had a single, 15-20 mm LPUS. Patients were split into two equal groups at random: Group B received RURS combined with laser fragmentation, and Group A received LUL.
Results: 100 patients who were included in the trial were split evenly between the two groups based on similar demographic information and stone criteria. Regarding patient demographics and stone criteria, both groups were similar. Group A had a substantially greater stone-free percentage (100%) than Group B (72%). There was a significant difference (p<0.001) in the operating duration, hemoglobin deficit, and ultimate stone-free rate between groups A and B. There was little difference in the two groups' conversation rates, mucosal injuries, ureteral perforations, complications, and length of hospital stay.
Conclusions: Compared to RURS, LUL is linked to a greater stone-free rate and fewer complications
Keywords: Proximal Ureteric Stone, Retrograde Ureteroscopy, Laparoscopic Ureter Lithotomy, Stone Free Rate
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, , Bangladesh. Email:  |
Ali SMY, Islam MS, Islam MS, Jahan S, Islam MR, Miraj AKA, The Outcome of Different Endoscopic Modalities in the Management of Large Proximal Ureteric Stone. Int J Med Res Rev. 2024;12(6):176-182. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1515 |
 |
 ©
©