Lymphocytic colitis: an Important but Underdiagnosed Cause of Chronic Diarrhoea in Adult Nigerians
Okonkwo K1*, Ojo O2, Betiku O3
DOI:https://doi.org/10.17511/ijmrr.2024.i03.03
1* Kenechukwu Okonkwo, Lecturer, Department of Medicine, University of Medical Sciences, Ondo, Nigeria.
2 Olusegun Ojo, Professor, Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University, Ileife, Nigeria.
3 Omolade Betiku, Lecturer, Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University, Ileife, Nigeria.
Introduction: Lymphocytic colitis is an important cause of chronic diarrhoea which is amenable to appropriate treatment which helps to reduce the morbidity and mortality associated with chronic diarrhoea. In Africa unfortunately, there is poor awareness of this treatable cause of chronic diarrhoea on account of a paucity of skilled experts necessary to make a diagnosis and implement effective therapy.
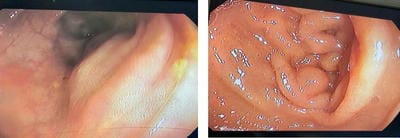
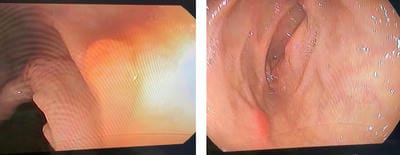
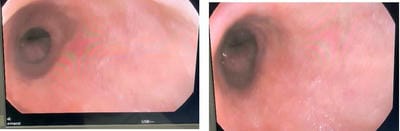
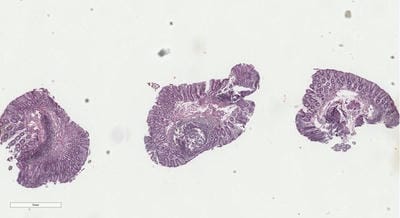
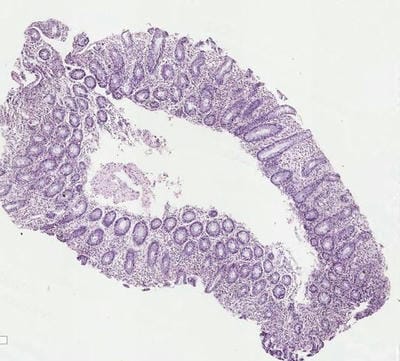
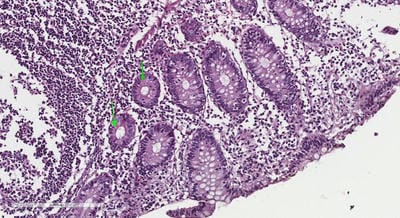
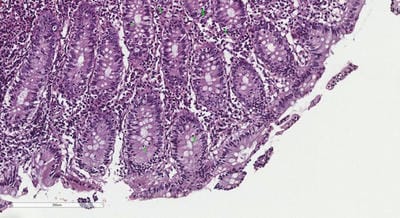
Aim: We present the clinical aspects, endoscopic findings and pathological features of twenty-one Nigerian patients with lymphocytic colitis. A short literature review of the epidemiological, clinical, endoscopic, and pathological features of this important condition is also presented.
Materials and Methods: This was a retrospective analysis of the clinical, endoscopic and pathological findings of twenty-one patients who were diagnosed with lymphocytic colitis following colonoscopy in an open-access endoscopy setting in Akure, Ondo State, Nigeria over eighteen months.
Results: Twenty-one diagnoses of lymphocytic colitis were made from a pool of one hundred and twenty-two colonoscopies done between December 2021 and May 2023. There were slightly more females diagnosed with an M: F ratio of 3:4 with a mean (SD) age of 52.2 (± 14.3) years. All of the patients had a history of passage of watery diarrhoea while normal colonoscopy findings were present in 87.5%. The mean (SD) time to diagnosis in five of these study subjects was 18.4 ± 9.1 months. These patients had standard medical treatment with good outcomes.
Conclusion: In sub-Saharan Africa, lymphocytic diarrhoea is a treatable cause of chronic diarrhoea. It is important to refer patients with chronic diarrhoea to facilities where they can benefit from the expertise of endoscopists and pathologists.
Keywords: Lymphocytic colitis, chronic diarrhoea, Nigeria
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Lecturer, Department of Medicine, University of Medical Sciences, , Ondo, Nigeria. Email:  |
Okonkwo K, Ojo O, Betiku O, Lymphocytic colitis: an Important but Underdiagnosed Cause of Chronic Diarrhoea in Adult Nigerians. Int J Med Res Rev. 2024;12(3):84-92. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1471 |
 |
 ©
©