4Dimensional XStrain Echocardiography assessment of Left Bundle Branch Cardiomyopathy in an elderly male: A case report
Mehrotra A1*, Shaban M2, Shakya U3
DOI:https://doi.org/10.17511/ijmrr.2024.i01.02
1* Akhil Mehrotra, Chief, Pediatric And Adult Cardiology, Prakash Heart Station, Nirala Nagar, Lucknow, Uttar Pradesh, India.
2 Mohammad Shaban, Cardiac Technician, Prakash Heart Station, Nirala Nagar, Lucknow, Uttar Pradesh, India.
3 Ujala Shakya, Cardiac Technician, Prakash Heart Station Nirala Nagar, Lucknow, Uttar Pradesh, India.
Left bundle branch block (LBBB) is generally associated with a poorer prognosis in comparison to normal intraventricular conduction. LBBB may be the first manifestation of a more diffuse myocardial disease. The typical surface ECG feature of LBBB is a prolongation of QRS above 0.11s in combination with a delay of the intrinsic deflection in leads V5 and V6 of more than 60 ms and no septal q waves in leads I, V5, and V6 due to the abnormal septal activation from right to left. LBBB may induce abnormalities in left ventricular performance due to abnormal asynchronous contraction patterns. Asynchronous electrical activation of the ventricles causes regional differences in workload which may lead to asymmetric hypertrophy and left ventricular dilatation, especially due to increased wall mass in late-activated regions, which may aggravate preexisting left ventricular pumping performance or even induce it.
Keywords:
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Chief, Pediatric And Adult Cardiology, Prakash Heart Station, Nirala Nagar, Lucknow, Uttar Pradesh, India. Email:  |
Mehrotra A, Shaban M, Shakya U. 4Dimensional XStrain Echocardiography assessment of Left Bundle Branch Cardiomyopathy in an elderly male: A case report. Int J Med Res Rev. 2024;12(1):12-21. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1461 |
 |
 ©
© 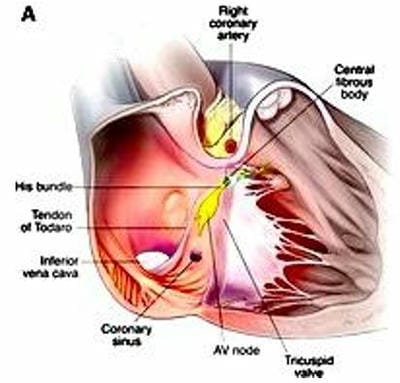
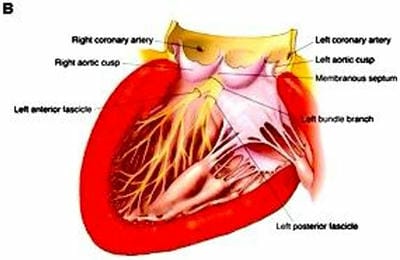 Figure 1: Anatomy of the cardiac conduction system and its relation to surrounding structures .
Figure 1: Anatomy of the cardiac conduction system and its relation to surrounding structures . Figure 2: Anatomy of LBB The left bundle branch comprises the main left bundle and distal anterior and posterior fascicles. LBBB from an incident disease requires a lesion just distal to the bundle of His (1) or extensive myocardial damage involving a large portion of the distal conduction system, including both the fascicles (2 and 3).
Figure 2: Anatomy of LBB The left bundle branch comprises the main left bundle and distal anterior and posterior fascicles. LBBB from an incident disease requires a lesion just distal to the bundle of His (1) or extensive myocardial damage involving a large portion of the distal conduction system, including both the fascicles (2 and 3).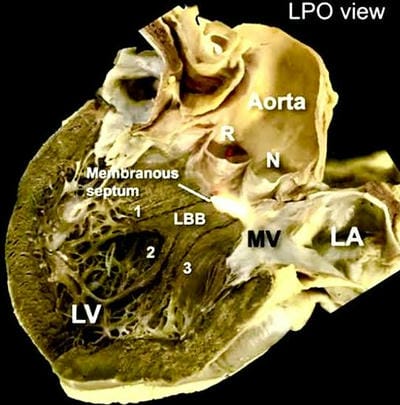 Figure 3: 4D tracking of the anatomy of the LBB The Left Posterior Oblique (LPO) view shows the trans-illuminated membranous septum located inferior to the interleaflet triangle between the right (R) and noncoronary (N) sinus of the aortic valve. Note that we have highlighted in dark color the limits of the endocardial position
Figure 3: 4D tracking of the anatomy of the LBB The Left Posterior Oblique (LPO) view shows the trans-illuminated membranous septum located inferior to the interleaflet triangle between the right (R) and noncoronary (N) sinus of the aortic valve. Note that we have highlighted in dark color the limits of the endocardial position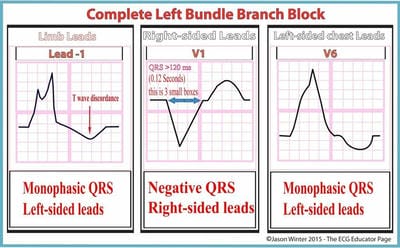 Figure 4: Diagrammatic representation of the ECG criteria of LBBB.
Figure 4: Diagrammatic representation of the ECG criteria of LBBB.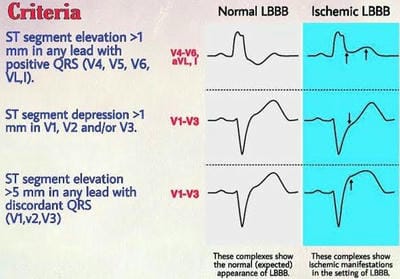 Figure 5: Diagramatic representation of ECG manifestations of ischemia on LBBB.
Figure 5: Diagramatic representation of ECG manifestations of ischemia on LBBB.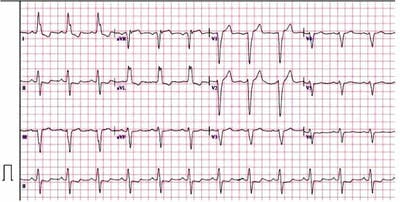 Figure 6: Resting ECG consistent with LBBB.
Figure 6: Resting ECG consistent with LBBB.  (A)
(A) (B)
(B) (A)
(A)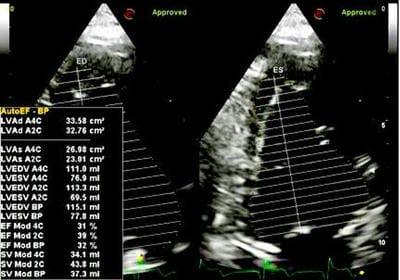 (B)
(B) (A)
(A) (B)
(B) Figure 10: LV endocardial volumes, 4D-EF%, cardiac output, and sphericity index.
Figure 10: LV endocardial volumes, 4D-EF%, cardiac output, and sphericity index.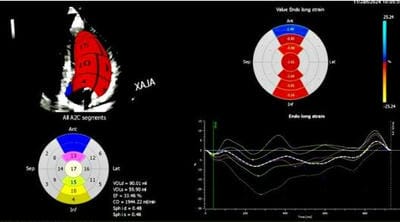 (A)
(A)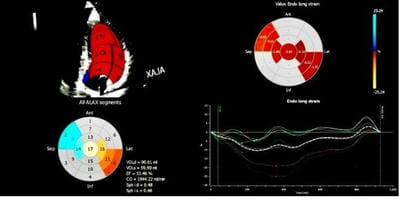 (B)
(B)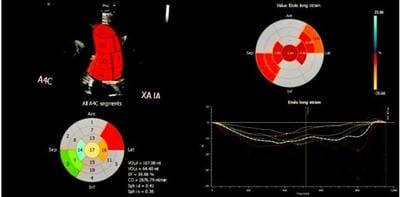 (C)
(C)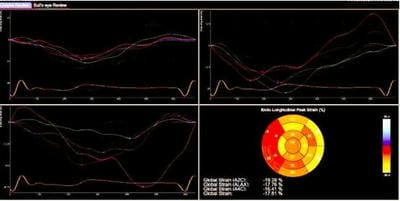 (D)
(D)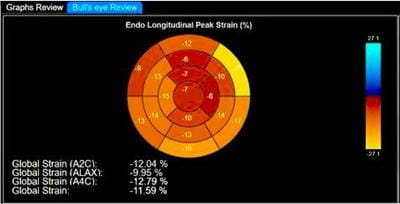 Figure 12: Global Longitudinal peak strain (%) of LV.
Figure 12: Global Longitudinal peak strain (%) of LV. (A)
(A) (B)
(B)