In Hospital Outcome of Acute Anterior Myocardial Infarction in Diabetic and Non-Diabetic Patients
Suhail Alam M.1*, Shahabuddin M.2, Abdul Mukid M.3, Tazin F.4, Tarin T.5, Sarathi Roy Chowdhury P.6
DOI: https://doi.org/10.17511/ijmrr.2023.i05.01
1* Md. Suhail Alam, Assistant Professor, Department of Cardiology, Jalalabad Ragib Rabeya Medical College, Sylhet, Bangladesh.
2 Md. Shahabuddin, Ex-Professor and Departmental Head (Cardiology), MAG Osmani Medical College, Sylhet & Vice Principal and Departmental Head (Cardiology), Parkview Medical College, Sylhet, Bangladesh.
3 Md. Abdul Mukid, Assistant Professor, Department of Cardiology, Parkview Medical College, Sylhet, Bangladesh.
4 Farzana Tazin, Senior Consultant (Cardiology), Clinical and Intervention Cardiologist, National Heart, Foundation Hospital, Sylhet, Bangladesh.
5 Tafhema Tarin, Junior Consultant, Department of Paediatrics, Sylhet Women’s Medical College & Hospital, Sylhet, Bangladesh.
6 Partha Sarathi Roy Chowdhury, Junior Consultant, Department of Cardiology, 250 Bed Adhunic Sadar Hospital, Hobigonj, Bangladesh.
Background: Patients with acute anterior myocardial infarction and diabetes have a poor prognosis. Objectives: To see the in-hospital outcome of acute anterior myocardial infarction in diabetic and non-diabetic patients. Methodology: This cross-sectional observational study was conducted in the Department of Cardiology, Sylhet MAG Osmani Medical College Hospital, Sylhet over two years from July 2015 to June 2017. A total of 100 acute anterior MI patients (50 diabetic and 50 non-diabetic) were included in this study. Acute anterior MI patients admitted after 6 hours of symptom onset or who did not receive streptokinase were excluded. Results: Hypertension was found more among non-diabetic [27 (54%) versus 19 (38%); p>0.05] but the difference was not statistically significant. Diabetic group had more Apical Anterior MI [22 (44%) versus 19 (38%); p<0.05] and Extensive Anterior MI [20 (40%) versus 11 (22%); p<0.05] while non-diabetic group had more Septal MI [10 (20%) versus 3 (6%); p<0.05] and Mid Anterior MI [10 (20%) versus 4 (8%); p<0.05]. LV ejection fraction was found significantly low in diabetic patients [43.96 ± 5.95 versus 53.68 ± 6.36; p<0.01]. Killip Class III was more in the diabetic [24 (48%) versus 9 (18%); p<0.01] and Killip Class I was more in the non-diabetic group [18 (36%) versus 3 (6%); p<0.01] according to Killip classification of HF which was statistically significant between the two groups. Atrial Fibrillation was more in diabetics [6 (12%) versus 1 (2%); p<0.05] while sinus tachycardia was more among non-diabetics [20 (40%) versus 5 (10%); p<0.05] which are statistically significant. The diabetic group had more acute MR [2 (4%) versus 0 (0%); p>0.05] but was not significant. Death was more pronounced in the diabetic group than in the non-diabetic group [7 (14%) versus 3 (6%); p>0.05] but it was statistically not significant. Conclusion: It is concluded from the present study that in-hospital outcomes of acute anterior myocardial infarction are worse in diabetic patients than in non-diabetic patients.
Keywords: Outcome, Acute Anterior Myocardial Infarction, Diabetic
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Cardiology, Jalalabad Ragib Rabeya Medical College, , Sylhet, Bangladesh. Email:  |
Md. Suhail Alam, Md. Shahabuddin, Md. Abdul Mukid, Farzana Tazin, Tafhema Tarin, Partha Sarathi Roy Chowdhury, In Hospital Outcome of Acute Anterior Myocardial Infarction in Diabetic and Non-Diabetic Patients. Int J Med Res Rev. 2023;11(5):101-108. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1441 |
 |
 ©
© 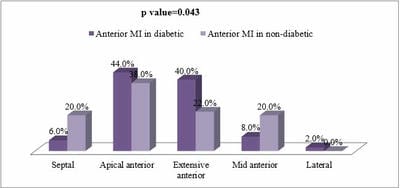 Figure I: Comparison of sub-classification of anterior MI between group A and group.
Figure I: Comparison of sub-classification of anterior MI between group A and group.