Acute Febrile Illnesses – Clinico-epidemiological Pattern in a Remote Geographical Location of North-eastern India
Monya M.1*
DOI: https://doi.org/10.17511/ijmrr.2023.i04.01
1* Michi Monya, General Duty Medical Officer, Chera Talo District Hospital, Kurung Kumey, Arunachal Pradesh, India.
Background: Acute undifferentiated febrile illness (AUFI / AFI) is a common cause for patients seeking hospital care in tropical countries like India. Non-specificity of symptoms and lack of appropriate diagnostics pose a challenge, especially in resource-limited settings. Investigation into the etiology and trends of AUFI provide valuable public health data to target clinical workup and guide optimal treatment. Method: A record-based descriptive study was conducted on all AFI cases presented to a Government tertiary care centre in a tribal hilly state of Northeast India in the year 2021. Result: Under five children were the most affected and respiratory infections were the most common cause of fever. Enteric fever and scrub typhus were the most common cause of undifferentiated fever. However, it was a remarkable finding that no case of malaria or dengue was reported from this region. Fevers remained undetermined in 28% of cases. Undetermined fevers and scrub typhus had higher occurrence during winters while no seasonality was observed with enteric fever. The majority of the patients recovered and were discharged. The case fatality rate was 0.35%. Conclusion: The local epidemiology of AUFI can help guide presumptive diagnosis and deliver optimal patient management in these settings. Typhoid and scrub typhus are to be considered differentials for AUFI in this region.
Keywords: Acute febrile illness (AFI), Acute undifferentiated febrile illness (AUFI), Epidemiology, Northeast India
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , General Duty Medical Officer, , Chera Talo District Hospital, Kurung Kumey, Arunachal Pradesh, India. Email:  |
Michi Monya, Acute Febrile Illnesses – Clinico-epidemiological Pattern in a Remote Geographical Location of North-eastern India. Int J Med Res Rev. 2023;11(4):82-88. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1429 |
 |
 ©
© 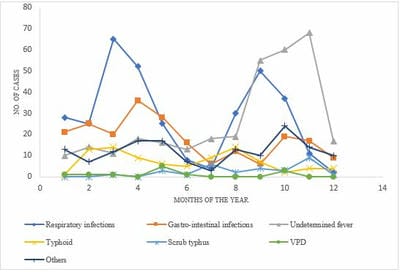
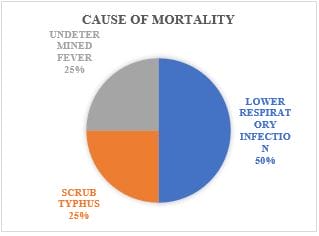 Figure 2: Causes of mortality, AFI cases, Govt. Tertiary care centre, Arunachal Pradesh, 2021
Figure 2: Causes of mortality, AFI cases, Govt. Tertiary care centre, Arunachal Pradesh, 2021