Randomized, Standard Controlled Study Evaluating the Efficacy and Safety of Habb-e-Waja‘al-Mafāsil in Managing Cervical Spondylosis
Husain S.1, Ahmad Rather S.2, Ahmad Bhat S.3*
DOI: https://doi.org/10.17511/ijmrr.2023.i02.02
1 Safia Husain, PG Scholar, Department of Moalajat, Regional Research Institute of Unani Medicine, Naseembagh, University of Kashmir, Srinagar, Jammu and Kashmir, India.
2 Shameem Ahmad Rather, Reader, Department of Moalajat, Regional Research Institute of Unani Medicine, Naseembagh, University of Kashmir, Srinagar, Jammu and Kashmir, India.
3* Shabir Ahmad Bhat, Assistant professor, Department of Moalajat, Regional Research Institute of Unani Medicine, Naseembagh, University of Kashmir, Srinagar, Jammu and Kashmir, India.
Background and Objectives: Cervical Spondylosis is a degenerative disease of intervertebral discs and adjacent vertebral bodies of the cervical region due to wear and tear changes. Neck pain, radiculopathy, and stiffness comprise the prime features of cervical spondylosis demanding immediate attention and respite. Despite the advancement in pharmacological, nonpharmacological and surgical interventions, the management remains unsatisfactory due to high cost, adverse effects and unusual eventualities. Hence a clinical trial was done to evaluate the efficacy of herbal formulation, Habb-e-Waja‘al-Mafāṣil (HWM), in managing cervical spondylosis (Waja‘al-‘Unuq). Methods: The study is an open-labelled, randomized and standard controlled trial. Sixty diagnosed patients of age group 20 to 70 years were randomly allocated, using a computer-generated chart, in the test group (n=30) receiving HWM (6gm), and the control group (n=30) receiving ibuprofen 1200mg/day, orally in divided doses. The severity score of clinical symptoms and signs; pain, stiffness, swelling, restriction of movement and radiological findings were analyzed at baseline and 30 days. Results: Both HWM and ibuprofen significantly reduced the severity score of pain, stiffness, swelling, and restriction of movement (p=<0.001) associated with cervical spondylosis after completion of the treatment protocol. However, no change was observed in radiological findings in either group (p=1). In comparison to the control group, no significant result was noticed in the test group statistically (p=>0.05), except for “restriction of movement” (p=<0.05). Conclusion: The herbal formulation, HWM, is equally effective as conventional treatment in managing cervical spondylosis. Therefore, HWM can be prescribed as a safe and cost-effective alternative treatment for cervical spondylosis.
Keywords: Herbal, Radiculopathy, Spondylosis, Unani
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant professor, Department of Moalajat, Regional Research Institute of Unani Medicine, Naseembagh, University of Kashmir, Srinagar, Jammu and Kashmir, India. Email:  |
Safia Husain, Shameem Ahmad Rather, Shabir Ahmad Bhat, Randomized, Standard Controlled Study Evaluating the Efficacy and Safety of Habb-e-Waja‘al-Mafāsil in Managing Cervical Spondylosis. Int J Med Res Rev. 2023;11(2):35-40. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1414 |
 |
 ©
© 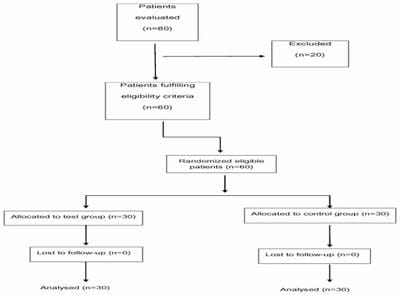 Figure 1. Patients summary (consort diagram)
Figure 1. Patients summary (consort diagram)